I. INTRODUCTION
Modern silicone breast implant was introduced in 1963, by Cronin and Gerow [1]. They report this implant as a ŌĆ£natural feelŌĆØ implant. Since the appearance of silicone gel, this has been a most common implant that is used in breast augmentation and reconstruction. As the use of silicone gel-filled implant increased, this implant evolved in several steps [1]. The implant that is used from 1964 to 1972 is classified as 1st generation implant. It had a thick gel and shell. It had Dacron patches on the posterior wall that helps to adherent to the chest wall. However, this patch contributed to make a severe distortion in capsular contracture. To improve the texture and to avoid the severe complication such as distortion of breast, 2nd generation implant had soft gel and wall. Although it overcame the weakness of 1st generation implant, soft shell and gel contents have a provisional risk of gel bleeding. In spontaneous rupture condition, less cohesive soft silicone gel is easily escape from the capsule. Leakage of silicone gel made a problem like a siliconoma. From the 1982, 3rd generation implant choose the cohesive silicone gel. This gel has a cross-linked silicone with long polymer side chains [2]. It is more cohesive than former generation gel and the leakage is decreased. It is clearly more durable than 2nd generation gel, however, the degree of consistency is little different among the manufacturers.
Foam stable silicone implant is categorized in 4th or 5th generation implant. The classification between 4th and 5th generation implant is obscure. In 3rd~5th generation gel, all the generation has cohesive gel filling and smooth texture, and polyurethane covered shell types. Only with the degree of cohesiveness, the generation is divided. Regardless of the generation, foam stable silicone gel implant came into the market since 1993 in Europe. Foam stable silicone implant is also called in ŌĆ£cohesive gelŌĆØ, ŌĆ£highly cohesive gelŌĆØ, ŌĆ£tear drop gelŌĆØ or ŌĆ£form stable anatomic shape gel.ŌĆØ Recently, in breast implant market, these neologisms make surgeons confused. In this article, we expect to look over the accurate definition about new generation silicone breast implant, and discuss about the effectiveness and adequate use of thisimplant.
ŌģĪ. DEFINITION AND CHARACTERISTICS OF HIGHLY COHESIVE GEL IMPLANT
As mentioned earlier, cohesiveness is important characteristics in recent generation of silicone implant. Cohesive means intermolecular attraction between like-molecule. Water particle (H2O) is composed of molecules of hydrogen and oxygen. Oxygen molecules can have a viscosity with two-hydrogen bond. With cohesive characteristic of hydrogen bonding, water can make a drop. Closely, saline implant also can be a kind of cohesive implant. Main issue of cohesive implant is not a composition but a degree of form stable nature. As the polymer chain become longer, viscosity and stability of the gel becomes higher [3]. Generally, cohesive gel implant means cross-linked silicone gel. The texture of cohesive gel is soft and natural, and the form of cohesive gel is easily deformed by its position or circumferential pressure. Highly cohesive gel implant 4 implies that has longer cross-linked chain than the general cohesive gel implant. It is firmer than usual cohesive gel and easily maintains its shape in any condition. For the reason, this implant is also called ŌĆ£form stableŌĆØ implant. Form stable implant means the implant that has capability to sustain the constant shape.
Up to this day, each corporation that produces breast implant has made such breast implant in name of ŌĆ£cohesive gelŌĆØ and ŌĆ£highly cohesive gelŌĆØ. However there are delicate differences in firmness and density between the products.
Understanding the importance of form stability of a gel implant is closely related to the shape of an implant. Implants can be made in a round shape orin a teardrop (anatomic)shape.
All four possibilities (Cohesive round, cohesive anatomic, non-cohesive round and non-cohesive anatomic) exist, but cohesive anatomic and non-cohesive types are the most common way that implants are manufactured. Anatomic implants are usually made out of form stable gel, round implants are made with a non-form stable gel.
Form stable round implants are used asŌĆ£salvage implantŌĆØ for thin tissues or loose pockets. However, these implants are used limitedly because they make breast lookssimilarto overinflated round saline implant,so called ŌĆ£BaywatchŌĆØ look.
In United State, many people and surgeons call this implant ŌĆ£gummy bear implantŌĆØ. Gummy bear is soft, elastic and flexible. At the same time, it retains consistent shape in any condition. When we cut the gummy bear, we can observe the each portion of this cut bear retain its original shape. Alike this delicious bear, this implant is sustained a constant form after being cut into small portions.
Ōģó. EFFECTIVENESS OF HIGHLY COHESIVE GEL
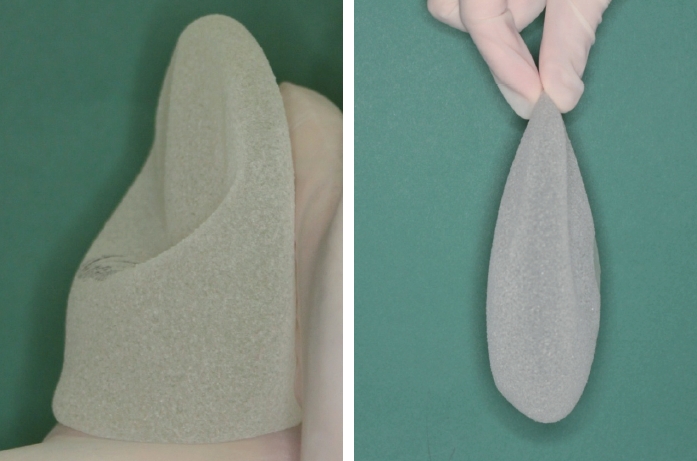
The biggest difference between non-form stable implant and form stable implant is the characteristic to sustain the constant shape under the breast parenchyma. This difference is showed in following simple test (Fig. 1). With loosely grasping the nonstable implant with hands, we can easily observe that implant upper pole filling is easily sunken. On the other hand, with tightly grasping, upper pole bulging can be observed.
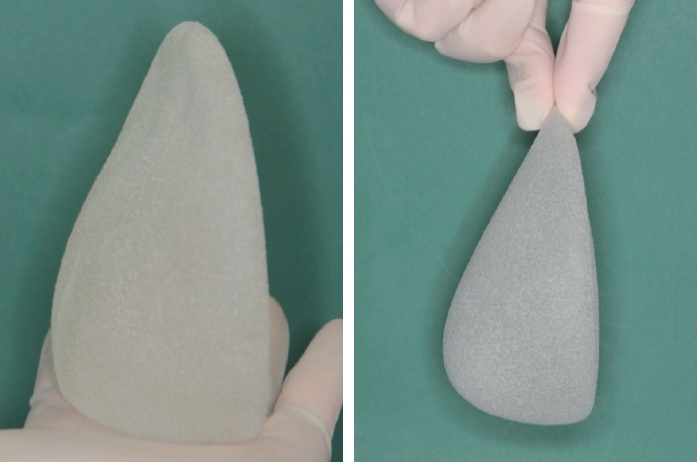
In same situation with hand grasping, form stable implant has a tendency to keep a consistent contour (Fig. 2). Form stable implant is easily predictable in the aspects of final contour and durability.
Fig. 3 shows this difference between form stable and nonform stable gel. With standing position, non-form stable gel is easily dropped in influence of gravity. In contrast, form stable gel implant keepsitsshape in upstanding position.
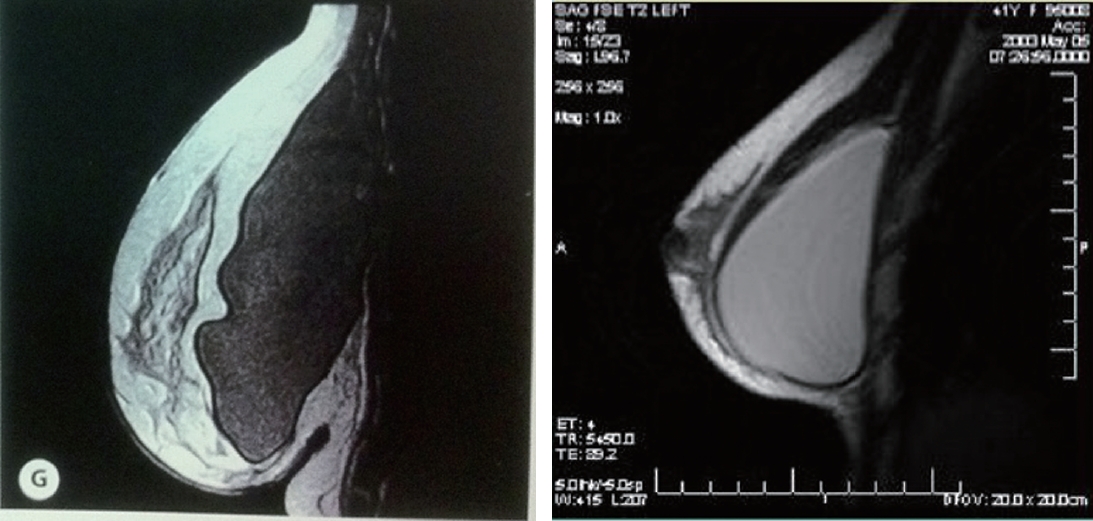
As for these findings, we suggest the change of implant after that is inserted under the breast. In long term follow up (2 years) of magnetic resonance image study of augmented breast, non-form stable anatomic shape implant gets out of its initial shape (Fig. 4) [4]. Non-form stable implant cannot overcome the weight of breast. The implant is molded by breast parenchyma. In this MRI finding, upper pole filling was collapsed and the upper border of implant changed in wavy shape. Because of the collapse of implant upper pole, the shape of upper breast is sunken. Correspondingly, lower breast appears overfill shape. Collapsed and folding implant may cause spontaneous implant rupture. Also, silicone leakage from the non-form stable implant provokes inflammatory reaction that brings about capsular contracture [5]. By contrast, with form stable implant, the implant shape did not change in long term follow up period. Form stable implant is stable and strong to overcome the breast weight and to mold the breast in constantshape. In other words , breast molds the non-form stable implant shape and the form stable implant moldsthe breast shape.
In cross-section of form stable implant, when examiner applied the finger press the portion, gel was bulging but when the finger press was removed, gel shape returned to initial shape without deformation (Fig. 5).
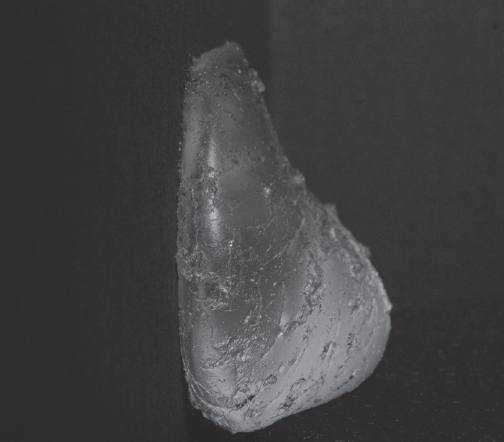
Even entire shell of form stable implant is peel off, the contour of gel is not changed (Fig. 6). Because form stable gel has a highly cohesiveness, it has ability to keep its original shape without thick implant cover. With this result, we predict that the gel bleeding phenomenon is extremely rare although implant rupture. Regardless of confused terminology like ŌĆ£CohesiveŌĆØ and ŌĆ£Form stableŌĆØ implant, the form stable nature is most important characterin these new generation silicone implant.
ŌģŻ. IMPLANT TYPE AND PROPER SELECTION
Natrelle TM style 410(Allergan Inc., Irvine, CA, USA) is the first highly cohesive form stable implant. Since Allergan introduce this implant in market in 1993, many corporations have manufactured similarimplant. MEMORYGEL TM CPGTM (Contour Profile Gel) (Mentor Worldwide LLC, Santa Barbara, CA, USA), Replicon┬« (POLYTECH Health & Aesthetics, Dieburg, Germany), Naturgel TM (Sebbin, Boissy-lŌĆÖAillerie, France) et al. are classified asform stable implant.
In style 410, there are 12 types of gel according to the degree of implant height and projection (Fig. 7). In traditional round gel implant, breast width is most important factor for selecting suitable implant size. Because non-form stable gel shape is eas ily molded in the body depending on patientŌĆÖs tissue tension, the projection of breast after augmentation is hardly predicted. The factors that decide the non-form stable device shapes are i) tissue envelopes tension surrounding the implant, ii) volumes that fills the implant, iii) degree of cohesiveness of silicone gel. However, in form stable implant, the anatomic shape of this implant is strong enough to endure the tissue tension; we can anticipate postoperative breast projection with ease. Implant projection and dimension is more important than implant volume in choosing the form stable implant. Considering patientŌĆÖs desire,surgeonsshould select an implant type [6].
Ōģż. CAUTIONS IN IMPLANTATION
To obtain a good result with form stable implant, surgeon must keep in mind following core points.
A. Tissue-based preoperative planning
To obtain successful result with form stable implant, obtaining data from preoperative chest wall and breast tissue measurement is important. Based on these data, proper implant selection and incision location are decided.
Implant projection should be decided in considering with glandular parenchyma amount [6]. Abundant breast tissue makes more central projection of breast and needs a small projection implant. In small breast that has natural and proper contour, round implant is suitable for augmentation. On the other hand, in patient who has poor breast shape like as constricted breast, form stable anatomic shape implant solves the problem of parenchymal maldistribution and improves both breast contour and volume. Also, alike the traditional breast implant, if Pinch test islessthan 2cm,retropectoral pocket dissection is advisable. Tissue characteristic must be reflected in preoperative measurement. In patients, who have lax skin, nipple-IMF distance tends to be underestimated. After breast augmentation with same size breast implant, the expanding skin amount between nipple-IMF islargerin lax skin type than tight one.
B. New inframammary fold (IMF) incision location
Incision location is also important decision point. IMF incision is favorable in augmentation mammaplasty using form stable implant. Many authors including Hëden [6] and Jewell [7] recommend IMF incision in this type implant. Asian patients tend to favor transaxillary incision with fear of breast hypertrophic hyperpigmented scar. However, IMF incision permits more precise pocket dissection, more cautious bleeding control and easy access of this firmer implant without rotation. To hide the scarin IMF incision, properincision location is important.
Form stable implant has ability to expand lower pole breast [8]. After implant insertion, nipple-IMF distance is more stretched in the case using form stable implant than traditional round implant. Inexperienced surgeons can make an unintended high IMF incision using form stable implant.
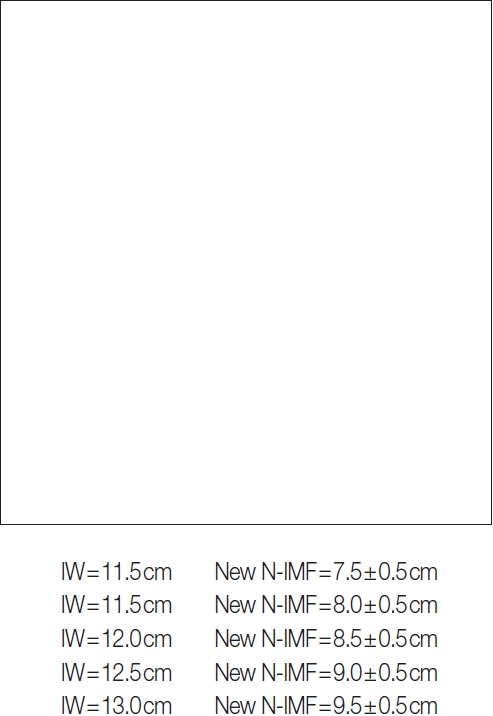
There are many methods to decide the new IMF position. Individually, authors prefer Randquist formula to others. In Randquist formula, the width of the implant (IW) generates a value for the new nipple-IMF distance and new IMF position (Fig. 8). In this formula, an implant with a 12cm width needs a lowering of the fold to 8.5cm (┬▒0.5cm). If 0.5cm is added to planed implant width, 0.5cm is added to IMF lowering. Also, if the patient has a lax skin, 0.5cm issubstracted from the calculated IMF lowering amount. On the contrary to this, if the patientŌĆÖ sskin istight, 0.5cm is added. Furthermore, patientŌĆÖs upper pole parenchyma is overthe 4cm, an additional 0.5cm is added.
C. Accurate pocket dissection
Dissimilarly with round non-form stable implant, implant rotation is a big problem in anatomic implant. If surgeon dissect too large pocket to implant size, the implant is able to rotate into pocket. In HedenŌĆÖs study [6] in the largest case using Style 410, they experience the implant rotation in 4.2 percent. In BengtsonŌĆÖs study [9] , implant malposition is major cause of reoperation after breast augmentation. Biocellsurface of Style 410 is effective to reduce the implant rotation [10]. Biocell surface is composed with diversely sized open-pores (100-600um). This texturized surface of Biocell allows tissue in-growth and adherence into this aggressive pore. Despite this nature of Biocell, implant rotation cannot be completely prevented. To avoid the reoperation, precise sizing isimportant in pocket dissection.
However, surgeons have to decide the pocket size cautiously because when the pocket is too small and strict in compare with implant diameter, the edge of implant may be palpable above the breast tissue.
Bengtson [4] compare the reoperation and complication rate of Style 410 highly cohesive gel to non-form stable gel in his study. He collected the data of 3 years follow up period in Style 410 and 4 years in standard silicone gel. In standard silicone gel, reoperation rate is 23.5 percent (n=455), implant rupture was 2.3 and capsular contracture grade III/IV was 13.2. On the other hand, in Style 410, reoperation rate was 12.5 percent, implant rupture was 0.7 and capsular contracture was 1.9. HedenŌĆÖs study 11 in 2006 also revealed lower implant rupture and contracture rate in Style 410 in comparison with traditional silicone gel implant. In his study, they observed6 Style 410 implants during 6 years with magnetic resonance image scan. In follow-up period, 0.3 percent of overall implant shows implant rupture sign in MRI (like linguini sign or inverted loop sign) and 0.7 percent of intermediate rupture sign can be detected.
With physical examination, capsular contracture rate (over the grade III) was 5.6 percent. These reported complication rates in highly cohesive gel were lower than in previous 3rd generation gel. Holmich12 studied 271 patients who underwent breast augmentation with 3 rd generation gel. In magnetic resonance image study, possible rupture rate was 6 percent. In considering these results, form stable implant has lower rupture rate than traditional implant.
Ōģź. CONCLUSION
Appearance of form stable highly cohesive gel silicone implant makes a migration to next generation in breast implant market. Someone still point out that this implant has several weaknesses [13]. Usually, to insert this implant, longer incision is demanded than traditional axillary incision. Also, to make a precise pocket for anatomical implant, learning curve period is needed in young surgeons, and it has a risk of rotation and is hardly used in re-operation.
Although these disadvantages of form stable implant, it provides an excellent result and gives a new opportunity in implant choice. This newer implant can make a predictable result with a high patient and offers superior result than previous generation silicone implant and it can makes a precise and safe result [7,11]. Bengtson [9] called this implant in ŌĆ£these next generation, highly cohesive implantŌĆØ and he said this implant lowers complication rates and elevates patientŌĆÖs satisfaction. As mentioned above, highly cohesive form stable silicone implant is more advanced generation silicone implant. To achieve a successful transition from previous generation to next generation of silicone implant, surgeonŌĆÖs education, discretion and effort to avoid the problems are needed.