INTRODUCTION
Calves can be easily seen in daily life and are an important part of the body contour. Asymmetric calves can develop from unbalanced distribution and deposition of fat and muscles between the legs. Calf asymmetry may be due to congenital factors, disease (e.g., poliomyelitis, cerebral palsy, or infection), spinal cord injury, or the effects of surgical treatment and may have severe adverse psychological and social implications. Generally, an asymmetric calf is diagnosed when the difference of the longest circumference between both calves is more than 2 cm. Several surgical methods have been introduced for the correction of an asymmetric calf. Implant insertion or fat injection is used to augment a hypotrophic calf. Selective neurectomy, liposuction, muscle resection, radiofrequency, and botulinum toxin injection are used to treat a hypertrophic calf. With the development of microsurgery, the authors planned to use a latissimus dorsi musculocutaneous free flap (LDMC free flap) with silicone implant to add calf volume to obtain natural calf contour.
The authors present the first successful case of correction of a severely asymmetric calf using an LDMC free flap and customized silicone implant.
CASE REPORT
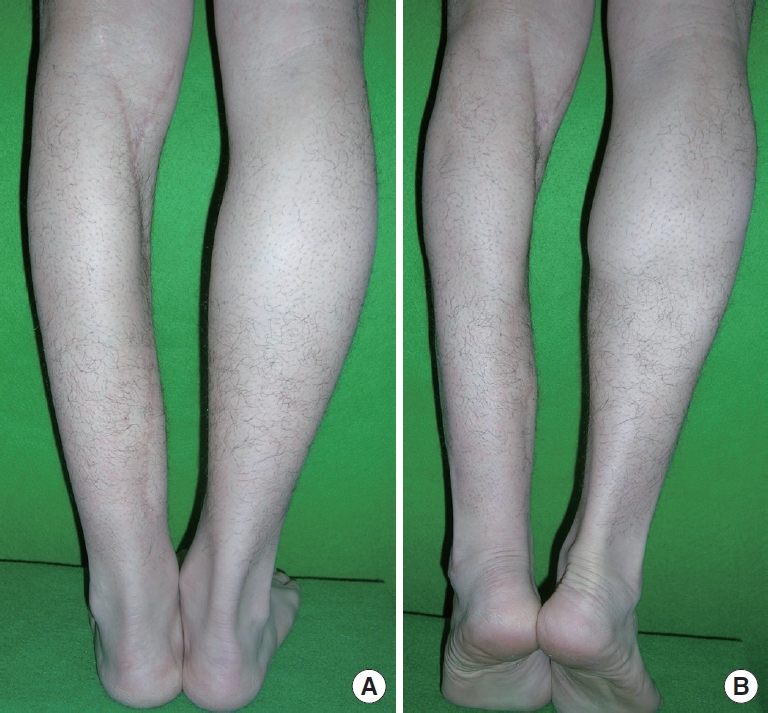
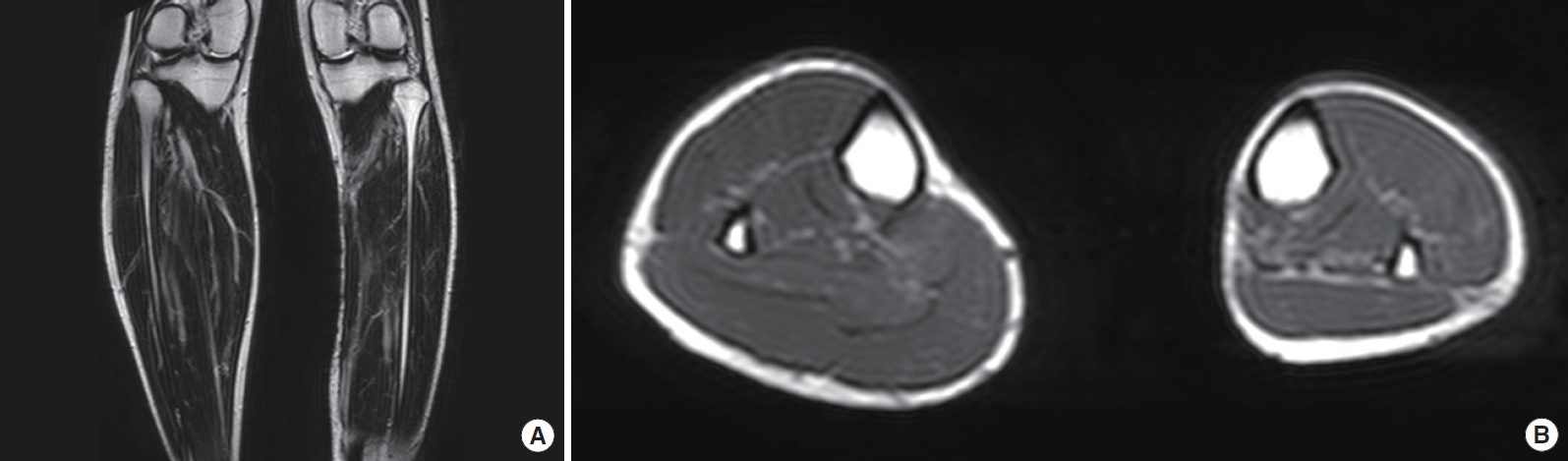
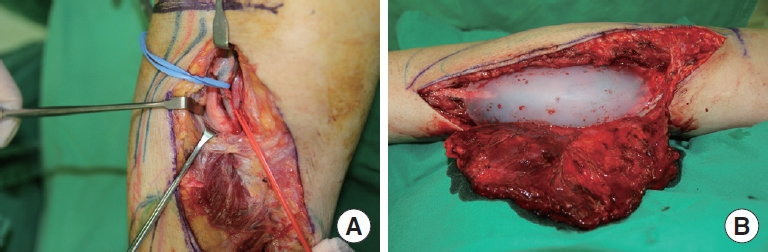
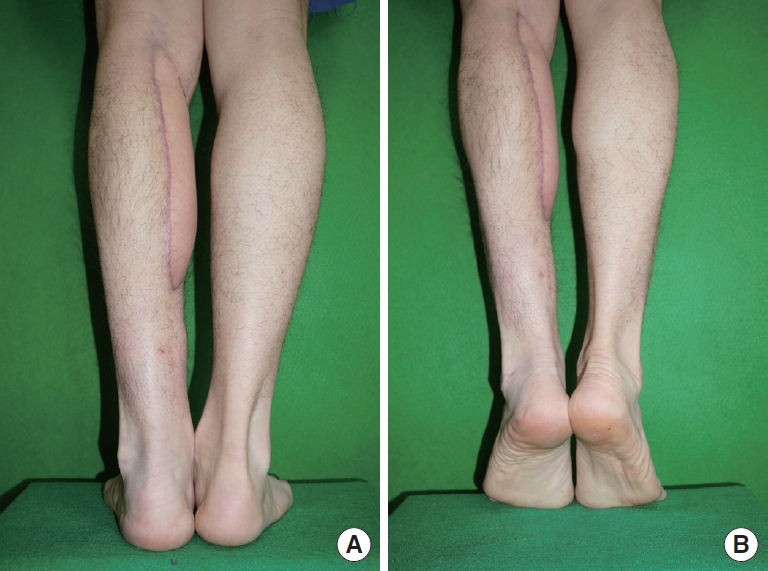
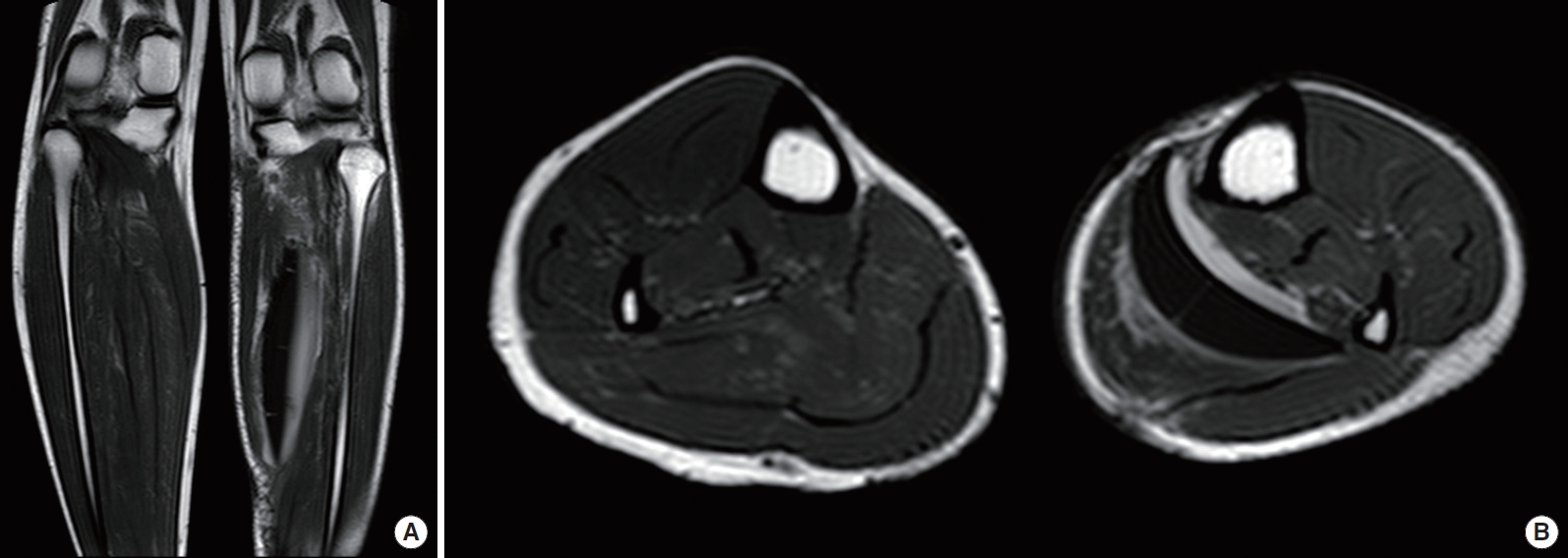
A 23-year-old man was diagnosed with EwingŌĆÖs sarcoma of the left lower leg in 2007. The man underwent en bloc resection of the medial side of the left lower leg and six courses of adjuvant chemotherapy and fully recovered. However, the patientŌĆÖs developed a severely atrophic depression deformity and a 20 cm long, wide depressed scar on the medial aspect of patientŌĆÖs left lower leg. Physical examination of the strength, shape, and balance of patientŌĆÖs legs, including toe and heel walking, showed no signs of functional problems, and he had a normal narrow base gait [1]. The authors measured the longest circumference of both calves. The calves were measured in the standing position and the tip-toe position before the operation. The circumference of the left calf was 30 cm and that of the right calf was 36.5 cm. The difference between both calves was 6.5 cm, which was included in the severe asymmetric group (Fig. 1) [2]. Before the surgery, the patient underwent magnetic resonance imaging (MRI) to obtain accurate anatomy and condition of the patientŌĆÖs calf muscles. There was a definite division of the medial and lateral side of the right gastrocnemius muscle. In contrast, there was severe atrophy of both the left soleus and left medial gastrocnemius muscles (Fig. 2). To augment the hypotrophic calf, the authors prepared a customized silicone implant for the patient before the operation. The mold of the implant was designed at the clinic. Afterward, the silicone implants were made in a factory (Keosan Silicone┬«, Keosan, Seoul, Korea) according to the mold. The implant was made of solid, middle-soft silicone [2,3]. Under general anesthesia, after making a 20 cm incision at the scar and careful subcutaneous dissection, the fascia overlying the flexor digitorum longus (FDL) muscle and flexor hallucis longus (FHL) muscle was identified. Careful dissection was required to identify the popliteal artery, vein, and tibial nerve (Fig. 3). The authors harvested a 21 ├Ś7 cm portion of LDMC free flap with a thoracodorsal artery. The thoracodorsal artery of the flap was anastomosed end-to-side to the popliteal artery. At the same time, two vena comitantes were anastomosed end-to-side to the two popliteal vein branches; the thoracodorsal nerve was anastomosed end-to-side to the tibial nerve as well. Finally, the customized silicone implant was inserted under the LDMC free flap and augmented to the medial aspect of the left hypotrophic calf. The circumference difference between the calves was reduced to 2 cm immediately after the operation. Three weeks later the circumference of the right calf was 35 cm and that of the left calf was 36.5 cm. Finally, six months later, swelling subsided and resulted in a 2.5 cm circumference difference between the calves (right-34 cm, left-36.5 cm) (Fig. 4). MRI after the operation showed no fluid collection and no dead space, and the latissimus dorsi muscle was well placed above the silicone implant (Fig. 5). About two weeks after the operation, the patient could ambulate, although he complained of gait disturbance. This gait problem seemed to be due to the implantŌĆÖs compression on calf muscles and postoperative inflammatory swelling [11]. However, the gait disturbance was temporary and improved within two weeks after operation. Therefore, the patient was educated to avoid severe activities for at least three months after surgery. The patient was satisfied with the natural calf contour and symmetry, and there were no complications such as inflammation or hematoma relating specifically to the implant insertion.
DISCUSSION
The legs are very important functional as well as sexually attractive parts of the body. In many countries, the legs account for a great part of the concept of physical beauty. Thus, patients often seek help from plastic surgeons to aesthetically enhance their calves. There are some commonly used surgical methods to treat this asymmetry. Implant insertion or fat injection is used to augment a hypotrophic calf, and selective neurectomy, liposuction, muscle resection, radiofrequency, or botulinum toxin injection is used to treat a hypertrophic calf [2-9]. It is known that a severely asymmetric calf is difficult to correct. In this case, the difference between the calves was 6.5 cm. Liposuction and selective neurectomy was initially planned on the right thicker calf, but the patient wanted only to augment the left thinner calf, as he complained of a tall and thin body type (height-182 cm, body weight-71 kg). The authors could achieve a circumference difference of 2 cm using augmentation with a silicone implant alone, so they decided to try a free flap using the patientŌĆÖs autologous muscle and skin overlying a silicone implant to obtain natural calf contour like medial bulging. A fat graft was actually planned to increase the circumference by another 2 cm but was not performed due to the patientŌĆÖs thin body shape. For more satisfactory augmentation, the authors used the customized silicone implant rather than the ready-made implants. Since the customized silicone implant fits well to each individualŌĆÖs calf shape and the base of the implant is designed concavely for minimizing the dead space when inserted, it can prevent significant side effects such as seroma collection or implant exposure [4]. The authors planned to use autologous muscle supplements in addition to the silicone implant, because excessive silicone implants can protrude through weak skin and the autologous muscle flap can prevent the silicone implant from protruding by covering the silicone implant. In addition, the autologous muscle flap presents a more natural calf contour than the silicone implant. Natural calf contour could be obtained by further immobilization and dressing with elastic bands and wearing pressure garments after surgery. Six months later, a 2.5 cm circumference difference between both calves remains. If liposuction and selective neurectomy on the right thicker calf was performed as planned with the patientŌĆÖs agreement, there would be little difference in the circumference between the calves. The reason why the authors decided to use the LDMC free flap among various free flaps is that it can provide a large muscle volume and an appropriately designed skin paddle that can be adjusted to the hypotrophic calf [10]. Until now, the free flap has been mainly used in reconstruction surgery; the authors used the free flap for aesthetic purposes to successfully correct a severely asymmetric calf.