INTRODUCTION
Lacrimal fistulas (LFs), also known as lacrimal anlage ducts, are supernumerary lacrimal canaliculi that connect the skin to the common canaliculus or the lacrimal sac [1,2]. In some cases, these may result from a secondary cause. However, most cases are congenital; therefore, congenital LF is the most accurate term for this condition [1]. The incidence of congenital LF is estimated to be 1 in 2000 births, and occasionally LF can be inherited in an autosomal dominant or autosomal recessive pattern [3-5]. LF is mostly unilateral and situated inferonasally from the medial canthus [6]. Some symptomatic cases may present with epiphora, blepharitis, or recurrent dacryocystitis, but most cases are asymptomatic, making treatment unnecessary [6]. Therefore, most patients with LF tend not to seek medical treatment for LF, unless they recognize that they have this condition.
Medial epicanthoplasty is a widely performed surgical procedure in East Asians because of their small and narrow nasal scleral triangle and their preference for large, balanced eyes. Medial epicanthoplasty using the skin redraping method introduced by Oh et al. [7] in 2007 is one of the most widely performed surgical methods. When carrying out this procedure on a patient with LF, the fistula may be included in the dissection range. In such cases, fistula management becomes important.
Herein, we introduce the case of a patient with LF that was found during medial epicanthoplasty and its management.
CASE
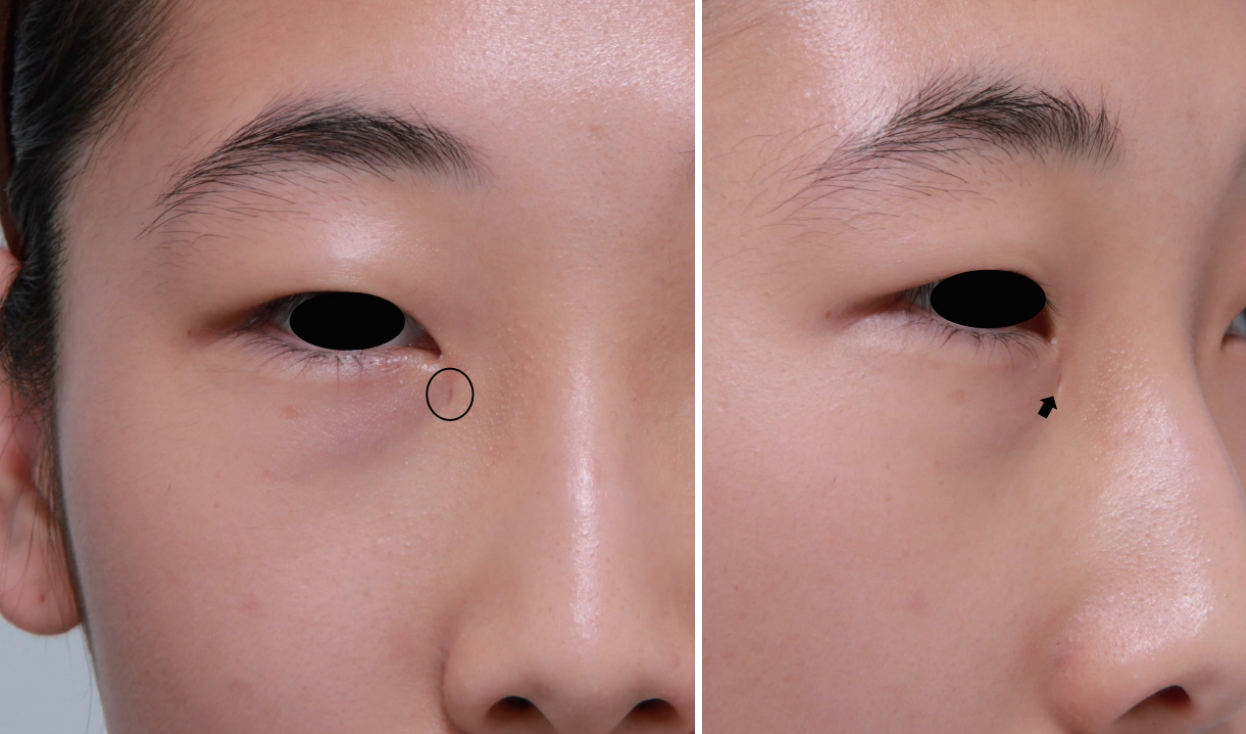
A 19-year-old woman visited our department to receive incisional blepharoplasty and medial epicanthoplasty. LF was found during a preoperative physical examination; it was located inferonasally from the medial canthus (Fig. 1). The patient did not exhibit any symptoms, including epiphora, mucoid discharge, or dacryocystitis. She underwent medial epicanthoplasty using the skin redraping method. During skin elevation in the midst of surgery, the fistula tract was detected. We cut off the fistula connected to the skin, and then cauterized the stump. Skin redraping and closure followed. However, 1 year after surgery, inflammation occurred in the same uneven area (Fig. 2). Moreover, hypertrophy of the remnant lacrimal duct occurred. Temporary improvement was observed upon the creation of an opening in the inflamed area followed by the administration of antibiotics, but the patientâs condition soon worsened. Thirteen months postoperatively, we created a fistula opening that reconnected the stump and the overlying skin. The wound remained stable over the course of 16 months of follow-up after this procedure (Fig. 3).
DISCUSSION
In addition to the rarity of LF, most patients with LF tend to be asymptomatic, which makes it difficult to detect this condition. The classification of congenital LF is based on the origin of its tract, which may be the common canaliculus, lacrimal sac, or the nasolacrimal duct [8]. If it originates from the common canaliculus or lacrimal sac, the fistula could be included in the skin flap during medial epicanthoplasty.
If LF is discovered during a preoperative physical examination, a diagnostic investigation is needed to accurately evaluate and detect its origin [8]. In adults, probing of the fistula or lacrimal irrigation to check for pharyngeal drainage is sufficient for a definitive diagnosis. However, a non-invasive test such as a fluorescein dye disappearance test is needed for evaluating children who cannot undergo invasive tests. If the dye stays in the eye, the duct can be considered blocked [9]. When conducting medial epicanthoplasty, it is preferable to detect the fistula by preoperative history-taking and a physical examination.
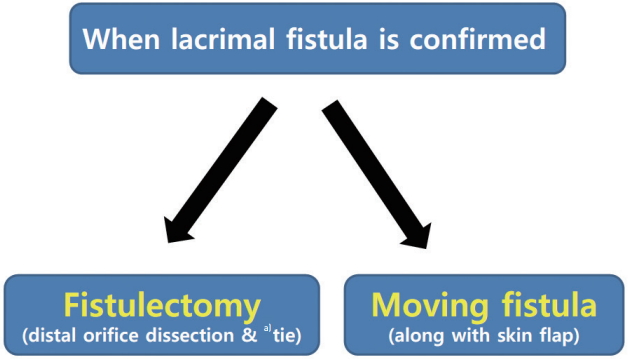
There are 2 ways to manage a fistula discovered within the dissection range during the medial epicanthoplasty procedure (Fig. 4). The definitive treatment is fistulectomy, which involves dissecting the tissue around the distal orifice of the fistula tract followed by tying the opening and separating the skin flap [6]. Since tying the opening of the fistula can sometimes block normal lacrimal drainage, one needs to check the patency of the normal lacrimal system by probing or irrigation after the procedure. When a small skin flap needs to be transferred during the medial epicanthoplasty, the opening of the fistula can be moved along with the skin flap [6]. In either case, it is extremely important to avoid only cutting or cauterizing the fistula tract because of the high recurrence rate of LF [6,8].
In conclusion, LF is an uncommon disease entity that physicians may encounter in clinical practice. Without prior background, not knowing how to manage this condition could be embarrassing. When LF is found during medial epicanthoplasty, the surgeon should not simply cut or cauterize the fistula tract because of the high recurrence rate of LF. Instead, fistulectomy should be preferentially considered, and the fistula can be moved along with the skin flap if a small skin flap is necessary for the transfer.