INTRODUCTION
The removal of unwanted body hair has recently become an increasingly prevalent trend, especially among women, and photoepilation by laser or other light-based technology has become one of the most popular noninvasive procedures performed in dermatology and plastic surgery [1].
Current laser treatments are based on the mechanism of selective photothermolysis, in which laser energy heats the target, allowing the surrounding structures to remain relatively intact. In laser hair removal, melanin in the hair shaft acts as the target chromophore for targeting hair follicles. Energy is transferred to the associated stem cells and follicular bulb, while selective cooling of the epidermis minimizes epidermal injury and damage to epidermal melanin [2]. Various wavelengths have been proven to target melanin in many studies. Suitable laser and light sources include intense pulsed light sources, ruby lasers (694 nm), alexandrite lasers (755 nm), diode laser systems (800 nm), and long-pulse neodymiumdoped yttrium aluminum garnet (Nd:YAG) lasers (1,064 nm) [3].
In the peer-reviewed literature, diode laser systems have emerged as the most effective hair removal method [4]. In this study, we used an 808-nm diode laser. A previous study histologically demonstrated that repetitive low-fluence laser devices induced necrosis in hair follicles. The aim of this study was to conduct a comparative evaluation of forearm and lower leg hair removal using an 808-nm diode laser at different fluences.
METHODS
Patient selection
The study was retrospectively approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital (2015-04-013). This was a prospective single-center, bilaterally paired, randomized comparison study. Twenty-four female patients were enrolled at Department of Plastic and Reconstructive Surgery of Soonchunhyang University Bucheon Hospital from February 2017 through May 2018. Patients who met the eligibility criteria were enrolled in this study. The inclusion criteria were as follows: age between 25 and 48 years, ability to comply with all study requirements, and willingness to refrain from using any other hair removal treatments during the duration of the study. The exclusion criteria of this study were as follows: age under 25 years or above 48 years; any signs of active localized or systemic infections; history of herpes simplex virus or acne scarring in the treatment area; allergy or photosensitivity; use of photosensitizing medications, minoxidil, isotretinoin, finasteride, or steroids; skin pigmentation disorders, ichthyosis, vitiligo, or psoriasis; pregnancy or plans to become pregnant; tattoos, chronic daylight exposure, or tanning; and having received other laser hair removal treatment for the axilla (within 20 weeks).
Study procedure
At the first visit, the hair count per square centimeter and hair follicle thickness were estimated on both axillae to determine the baseline values before treatment, and the first treatment was performed. All patients then received three treatment sessions, with a gap of at least 1 month between each session. In general, hair removal laser treatment was done at intervals of 1 to 2 months, and we established a minimum interval of 1 month. In all patients, an area measuring 2.5×2.5 cm was used to determine the baseline hair density. The ratio of the number of hairs before and after laser treatment was calculated. We used an 808-nm diode laser system (HR808 prototype diode laser; Wontech, Daejeon, Korea) in this study. Before treatment, a water-based lubricating gel at an ambient temperature was applied for epidermal protection as a heat sink. Hair trimming was done to a uniform length of 1–2 mm using safety scissors. Both axillary areas were divided into upper and lower parts. Each part was treated with a different fluence: 8 J/cm2 on the right upper part, 10 J/cm2 on the right lower part, 12 J/cm2 on the left upper part, and 14 J/cm2 on the left lower part. Laser pulses were given with two to four passes and emitted at a fixed rate of 5 Hz. The exposure duration time was 40 milliseconds in all areas. The spot size of our instrument was 10×10 mm. The mean time interval between successive pulses was 1–2 seconds. The clinical endpoint of treatments was the presence of slight perifollicular erythema.
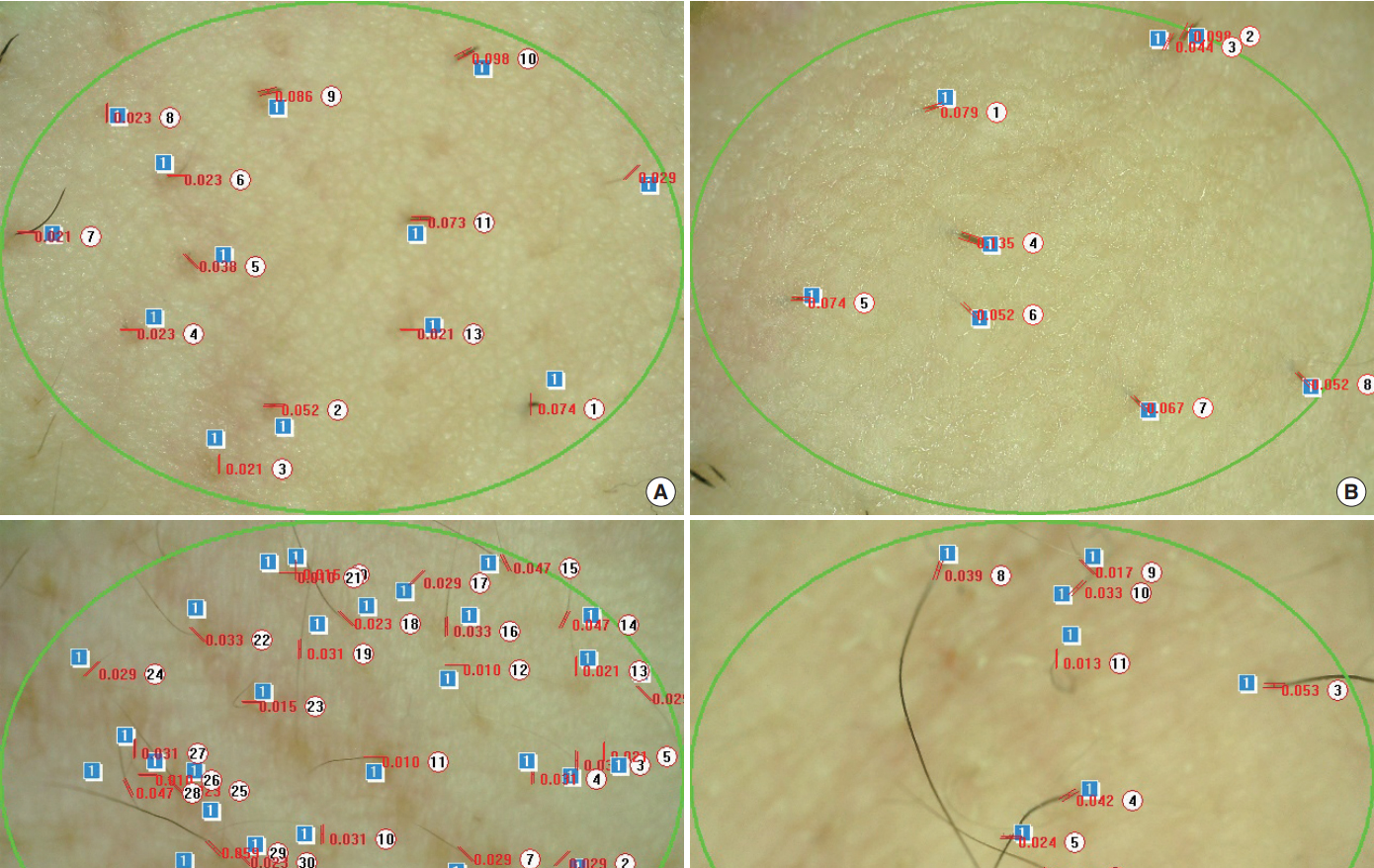
After each session, digital photographs (Nikon D750, Tokyo, Japan) were performed prior to the laser treatment in a photographic room. For each photo, identical ambient lighting, camera settings, and patient positioning were maintained. A standardized view with a fixed distance of 100 cm was used. Follicle thickness and density of the hair were assessed using a folliscope (Fig. 1). The results were evaluated 3 months after completion of the final treatment session.
The intensity of pain was subjectively expressed by each patient and recorded after each treatment. Pain was assessed using a visual analogue scale (VAS) for pain (0–10: 0, no pain; 10, worst possible pain). Therapeutic outcomes were assessed by patients’ satisfaction with the treatment results, which was evaluated using the following 4-point grading scale. At the 3-month (visit 5) follow-up visit, all subjects rated their satisfaction as excellent (3), very good (2), good (1), or fair (0). Independent clinical assessments of the treatment areas were conducted by three plastic surgeons who were blinded to the laser protocol based on comparative photographs using the following 5-point grading scale: 0, no change; 1, slight improvement (≤25%); 2, moderate improvement (26%–50%); 3, significant improvement (51%–75%); 4, excellent improvement (>75%). The final score of the physicians’ assessment was determined by the median value of the three scores for each patient (Table 1).
Statistical analysis
SPSS version 14.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Repeated-measures analysis of variance was performed to compare the changes in measured values over time among the four groups. P-values <0.05 were considered to indicate statistical significance.
RESULTS
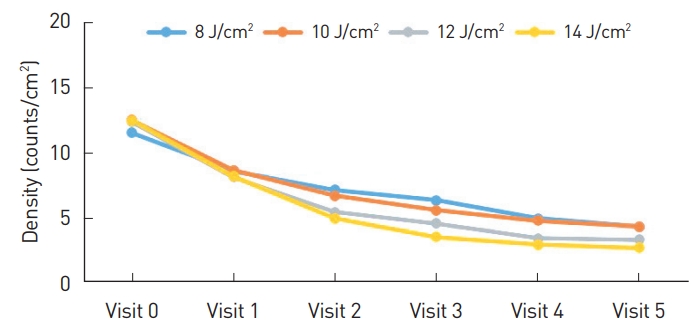
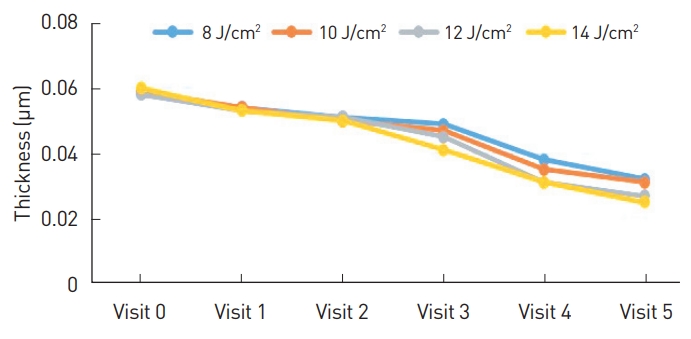
The study population comprised 24 subjects who visited our clinic for axillary hair removal. Their average age was 32.8 years (range, 25–48 years). Based on a comparison of data from the first visit and the final visit (3 months after treatment completion), the mean hair follicle density reduction was 62.18%, 65.28%, 73.08%, and 78.29% on the right upper side, right lower side, left upper side, and left lower side, respectively (Table 2). The mean hair follicle thickness reduction was 45%, 48%, 54%, and 59% on the right upper side, right lower side, left upper side, and left lower side, respectively (Table 3). The density and thickness changes were statistically significant in each group, but there were no statistically significant intergroup differences (P<0.05).
The VAS pain scores were 2.24, 2.29, 3.08, and 3.49 for the right upper side, right lower side, left upper side, and left lower side, respectively. The plastic surgeons’ assessment scores were 2.71 for both the left upper and lower sides, 2.38 for the right upper side, and 2.04 for the right lower side.
Some patients reported a slight heating sensation during the treatments, but indicated that it was tolerable. After the treatments, perifollicular erythema occurred and disappeared within 10 hours. There were no side effects such as burn injury, rash-like lesions, skin atrophy, or changes of pigmentation (hypopigmentation or hyperpigmentation).
DISCUSSION
In the modern world, the growth of hair in anatomic areas that are not cosmetically desirable is a common aesthetic problem. The methods of removing unwanted body hair include shaving, plucking, waxing, and chemical epilation. However, these methods yield temporary results. Laser hair removal was introduced in 1996 by Grossman et al. [5], who reported that ruby lasers had a hair removal effect. Laser hair removal has subsequently proven to be a comfortable and effective method, as confirmed by many clinical studies in the literature [6-8].
Numerous clinical studies have reported that diode lasers provide a safe, fast, and comfortable platform that can be used to manipulate a wide range of fluences, making them suitable for use on hair throughout the body [9]. Diode and neodymium-doped yttrium aluminum garnet (Nd:YAG) lasers have few and transient side effects, such as hyperpigmentation and pain, with skin types III to V because epidermal melanin absorption is lower for long-wave-length lasers [4]. Several previous clinical trials have compared the efficacy of hair removal between diode and Nd:YAG lasers in patients with darker skin types. Li et al. [10] compared the efficacy of diode and Nd:YAG lasers for axillary hair removal in Chinese women, and found that after two sessions, the hair reduction rate of the diode laser system was 78.56%, whereas a reduction rate of 64.50% was observed for the Nd:YAG laser. Bouzari et al. [11] also studied the difference between Nd:YAG and diode lasers for hair removal on the face and neck. The mean hair reduction was 42.4% and 46.9% for Nd:YAG and diode lasers, respectively. Furthermore, the mean number of laser treatment sessions was 2.6±1.2 for patients who underwent diode laser treatment, which was significantly lower than that of patients who underwent Nd:YAG laser treatment (5.5±2.2 sessions). In terms of treatment comfort, Eremia and Newman [12] noted that lasers with longer wavelengths caused more pain than lasers with shorter wavelengths. Youn et al. [13] reported that in Koreans, the most common skin type was type III (48.8%), followed by type IV (22.2%) and type V (17.8%). Based on the abstract of [13] a tendency was also found for skin types IV and V to become more frequent with advancing age. Therefore, because few studies have reported the efficacy of diode laser treatment in Korean patients, we evaluated diode laser treatment in Korean women. For our instrument, the manufacturer’s fluence guideline for the axillary area was over 8 J/cm2. Therefore, to investigate the optimal treatment parameters, we utilized a range of fluence levels, starting at 8 J/cm2 with slight increases.
Many studies have investigated the relationships of fluence and repetition rate with treatment effectiveness in diode laser treatment. Recent studies of diode lasers have suggested a shift away from the previously standard high-fluence devices in favor of a low-fluence (5–15 J/cm2) approach [14]. Braun [15] and Koo et al. [16] described a dramatic decrease in therapy-related pain and good efficacy after the use of low fluency 810-nm lasers with a high average power and a multiple-pass technique. Pai et al. [17] compared two 810-nm diode laser machines with different fluence levels and repetition rates for facial hair removal. They reported that a mode with low fluence (10 J/cm2) and a high repetition rate (10 Hz) was more efficient and caused less pain than a mode combining high fluence (25–35 J/cm2) with a low repetition rate (2 Hz). Li et al. [18] also compared different fluence levels and repetition rates of using an 810-nm diode laser for axillary hair removal in Chinese women. They reported that a low fluence (10 J/cm2) and a high repetition rate (10 Hz) had greater efficacy and less treatment discomfort than a mode combining high fluence (34–38 J/cm2) with a low repetition rate (1 Hz).
In our study, a different tendency was observed. For the objective parameters (hair density and follicle thickness), higher fluence was associated with higher overall mean reduction rates of density and follicle thickness (Figs. 2, 3). However, there was no statistically significant difference among the four groups. We think that our findings likely occurred as a result of the small number of enrolled patients and the smaller gap in the fluence parameter than in other studies.
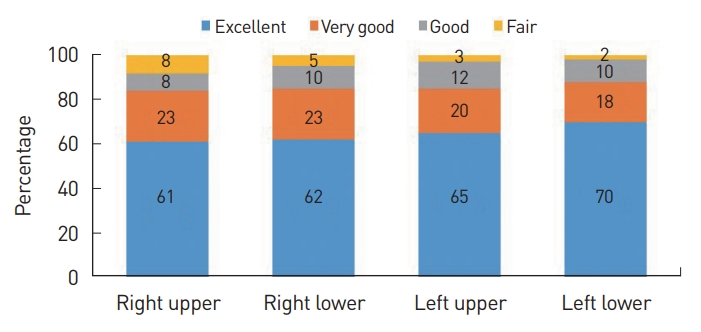
The majority of patients were satisfied with their treatment, as 80% of patients provided a response of “excellent” or “very good” (Fig. 4). The same tendency was shown for higher levels of the fluence parameter to be associated with a higher rate of “excellent” responses (Fig. 5). In the visual assessment by plastic surgeons, the scores for the left side (12–14 J/cm2) were higher than those of the right side. On the right side, the right upper side (10 J/cm2) received a higher score than the right lower side (8 J/cm2). The pain score was higher for the left side, but the difference between sides was slight.
In comparison with the findings of other studies, one of our noticeable results is that the parameter of “high” fluence was much lower than that of other comparative studies. Theoretically, lowering the fluence should reduce the pain resulting from the treatment. The pain caused by laser treatment may be influenced by many factors, such as the laser parameters (fluence, wavelength, and pulse duration), treatment site, and skin cooling technique. Rogachefsky et al. [19] reported that pain was directly related to longer pulse duration and higher fluence, and that complications were most severe in patients treated with the highest pulse duration and fluence. However, in our study, the pain score of the highfluence is similar to that of the low-fluence groups in other studies [17,19], and long-term complications were not investigated. Another difference is that we used a small number of pass technique, whereas the low fluence treatments in other studies used a multiple pass technique; a small number of pass technique was used in this study in order to reduce the time required for the treatment.
The axillary area is very sensitive to pain, and the patient must maintain an uncomfortable position during treatment in comparison with hair removal at other sites. Therefore, in addition to the effects of treatment, patients’ satisfaction is important factor in promoting adherence to the treatment regimen. Therefore, we suggest that the high level of fluence in our study (14 J/cm2) is advantageous in terms of patients’ comfort and adherence to treatment. We obtained a slightly better treatment effect than the conventional low-fluence treatment, while maintaining a similar level of comfort. Furthermore, our treatment time was shorter than that of the low-fluence treatments in other studies due to fewer number pass technique than other treatment regimen.
In conclusion, the high-fluence mode (14 J/cm2) efficiently removed unwanted axillary hair. This mode also significantly reduced the treatment time compared to the low-fluence mode of the diode laser system, with similar comfort and higher patient satisfaction. Therefore, for axillary hair removal with a HR808 prototype diode laser, the high-fluence mode is better than the low-fluence mode. Further studies with more patients will be necessary to verify whether a statistically significant difference is present.