INTRODUCTION
Frontal sinus fractures are common traumatic head and neck injuries that account for 8% of facial fractures [1]. Although there is no consensus regarding the ideal method of managing frontal sinus fractures, generally accepted indications for open reduction include a depressed anterior wall fracture, a displaced posterior wall fracture, or a nasofrontal duct injury [2]. Herein, we describe the treatment of a patient with a combined comminuted depressed skull fracture (FCCD) and naso-ethmoid-orbital (NEO) fracture that required open reduction. Since every component of the nasofrontal angle had been violated, accurate reduction based on adjacent bony landmarks was challenging, and a certain degree of postoperative deformity was anticipated. The authors devised a method for reconstructing the frontal bone and correcting the contour deformity using a pericranial flap.
CASE REPORT
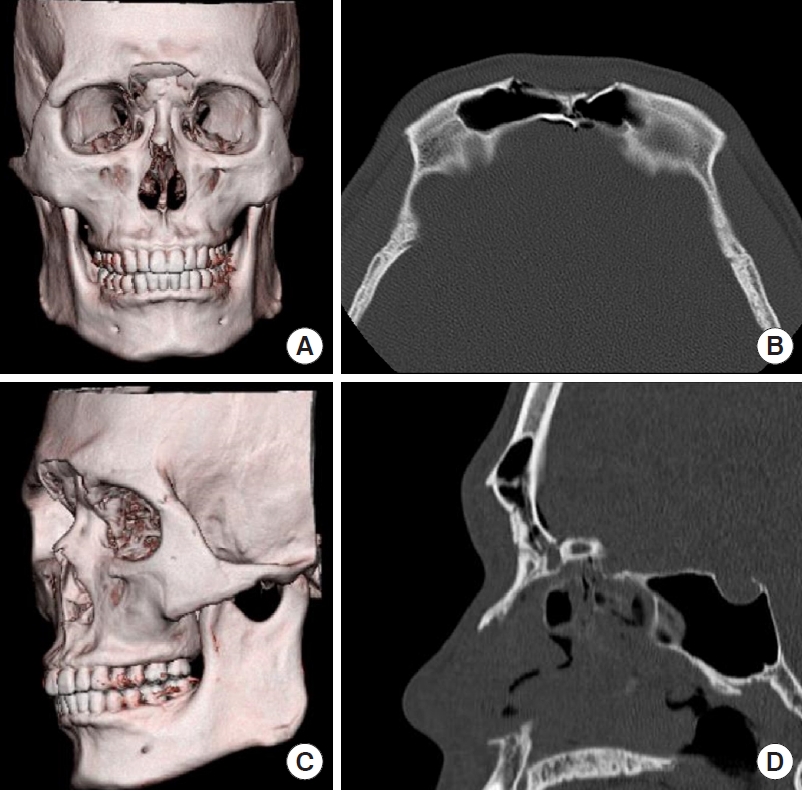
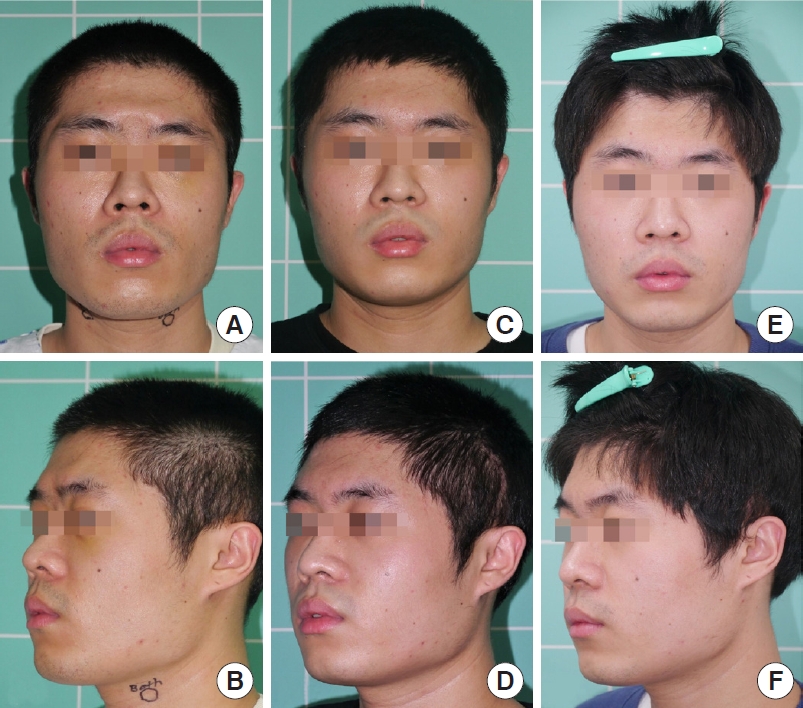
Preoperative computed tomography imaging of a 26-year-old male patient revealed an FCCD with NEO fracture resulting in a severe depression of the forehead (Fig. 1). An open coronal approach through the subgaleal plane was performed. The integrity of the pericranial layer was preserved. Following the coronal flap dissection, an anteriorly-based pericranial flap was elevated in a conventional manner. The width of the flap was designed to encompass the total length of both brows, and the length was designed from the start of the coronal incision, thereby maximizing the size of the flap that could be harvested. Reduction of the fractured frontal bone was completed with the insertion of an absorbable mesh plate (Resorb X; KLS Martin, Freiburg, Germany). The pericranial flap was folded in multiple layers with a width corresponding to the desired volume of the brow ridge (Fig. 2) and then fixed to the adjacent tissue with 5-0 Vicryl sutures. The folded pericranial flap along the brow ridge resembled a folded carpet for exhibition (Fig. 3). After reducing the facial fracture and applying the pericranial flap through this method (dubbed the ŌĆ£Persian carpetŌĆØ method), an adequate forehead contour and brow volumization were achieved (Fig. 4).
DISCUSSION
The utility of pericranial flaps has been proven in a wide range of craniofacial reconstructions. Pericranial flaps are commonly used for skull base reconstruction and cranialization or obliteration of the frontal sinus [3]. Their reliability is based on a robust blood supply from the supratrochlear and supraorbital arteries when anteriorly based [4]. As documented in numerous published reports, the versatile range of pericranial flaps spans from treating frontal sinus fractures to reconstructing the ear, forehead, orbit, and nose [5]. The most widely established use of pericranial flaps in craniofacial surgery is for obliteration of the frontal sinus. An anteriorly based flap is raised and folded into the entire sinus cavity to seal it off from the nasal cavity [6]. Nonetheless, the mainstay of pericranial flap usage relies upon the length and abundant volume of these flaps. Numerous studies have described the use of pericranial flaps in diverse situations, and have reported folding the flaps to achieve sufficient bulk. However, no previous studies have focused on augmenting the brow ridge, which is commonly violated after frontal sinus fractures.
The authors believe that the present method can be applied to patients with complex frontal sinus fractures without the need for obliteration. Optimal bony reduction will result in an inadequate restoration. However, when a combined FCCD and NEO fracture occurs, accurate reduction is not always achievable. In particular, if the patient strongly prioritizes aesthetic outcomes after surgery, an ancillary method for brow augmentation is required. The authorsŌĆÖ focus was to restore the nasofrontal angle and enhance the brow line. Using the Persian carpet method, the authors could accurately tailor the width of the flap to fit the patientŌĆÖs brow line. Camouflage of the inserted implant and fracture site was achieved, as well as augmentation of the brow ridge with adequate volumization. Furthermore, the flap could be elevated during the reduction procedure, so no additional donor site was required. Since an anteriorly based vascular flap was used, preservation of the original volume is predicted. The primary limitation of this study is that the method has been applied in only one case. However, based on our observations, the Persian carpet method can be used to overcome the risk of facial deformity in patients with compound facial fractures, including combined FCCD and NEO fractures.