INTRODUCTION
Radiation therapy is frequently used to treat breast cancer in conjunction with surgery and chemotherapy. The high-energy rays used in radiation therapy destroy cancer cells, but can also cause early and late radiation-induced soft tissue injuries in healthy tissue, mediated by reactive oxygen species [1]. One of the most serious complications of radiation therapy for breast cancer treatment is chest wall osteoradionecrosis [2,3], which is usually accompanied by ulceration, full-thickness skin necrosis, superimposed infection of the soft tissue and bone, and in severe cases, rib fractures [4].
Because of radiation-induced tissue damage in the skin and soft tissue around the necrosis, wide debridement and coverage with a well-vascularized flap are required for the treatment of osteoradionecrosis [5]. However, this is highly challenging in the chest wall for the following reasons: first, the use of local flaps is limited by the extensive radiation-induced skin and soft tissue changes around the area of necrosis. Second, in free flaps, recipient vessel candidates could be affected by radiation injury. Third, there is a limit to performing wide resection of the injured ribs and sternum since these are essential for a functional respiratory system.
Radiation-unaffected contralateral breast tissue can be a useful source of local flaps for the coverage of extensive chest wall wounds. There is a paucity of literature regarding the use of contralateral breast tissue for the reconstruction of chest wall defects. We present our experience with chest wall osteoradionecrosis treated with a contralateral breast Y-V flap.
CASE REPORT
Four years ago, an 81-year-old female patient presented with an open wound with a diameter of 1 cm accompanied by discharge on the right chest wall. One year ago, an increasing wound size along with turbid discharge caused the patient to be referred to our department (Fig. 1). Twenty-one years ago, the patient had undergone a modified radical mastectomy with axillary lymph node dissection for breast cancer in the right breast, followed by radiation therapy (20.94 Gy in 33 fractions). A computed tomography scan of the chest and bone scan revealed osteomyelitis in the right third to sixth ribs, further confirmed by bone biopsy. The patient’s final diagnosis was osteoradionecrosis accompanied by osteomyelitis and abscess. Methicillin-susceptible Staphylococcus aureus was identified from the wound culture, and levofloxacin was administered intravenously. Under general anesthesia, the radiation-induced fibrotic tissue around the wound was removed, and the right third to sixth ribs were partially excised, resulting in an open wound with an area of 113 cm2 (Fig. 2).
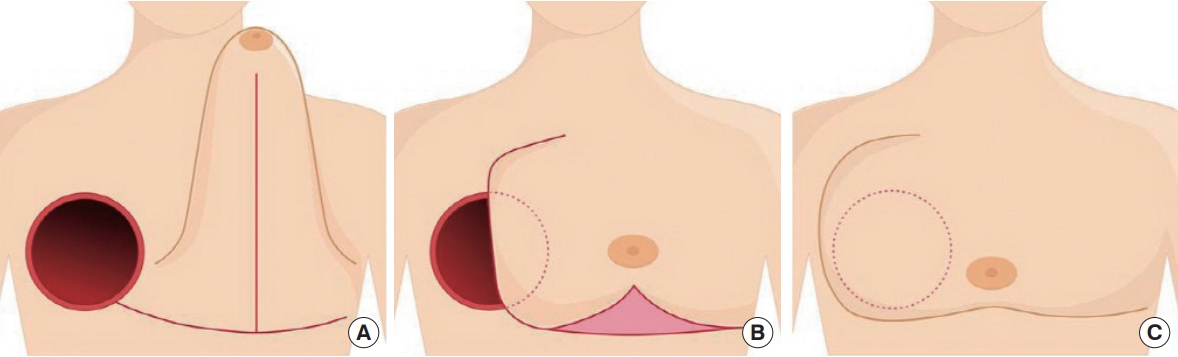
The contralateral breast had grade 3 ptosis with a length of 18 cm from the inframammary fold to the nipple-areolar complex. Reconstruction was performed to cover the open wound of the chest wall using redundant contralateral breast tissue. The flap was elevated in the subfascial plane after an inverted-T incision was made in the lower pole and inframammary fold of the contralateral breast, while preserving the perforators of the left lateral thoracic artery. The flap was spread in the Y-V advancement fashion to cover the open wound (Fig. 3). Two surgical drains were inserted under the flap (Fig. 4). The operation took 1 hour and 50 minutes.
Immediately after surgery, the patient’s vital signs were stable, with no signs of congestion or ischemic signs in the flap. On the sixth day after surgery, there was no necrosis of the flap. Partial dehiscence was observed in the right costal margin, which was the distal side of the flap, and an additional 8 cm2 local transposition flap was performed. No other complications were observed. The patient was discharged after the removal of sutures two weeks after surgery. No complications or ulcer recurrence was observed 19 months after surgery (Fig. 5). The patient was satisfied with the rapid recovery and surgical outcomes.
DISCUSSION
In breast cancer, radiation therapy is an important treatment for controlling local recurrence [6]. Despite advances in radiation therapy, complications such as osteoradionecrosis persist. Osteoradionecrosis mainly occurs in the mouth after radiation therapy for head and neck cancers. Although rare, it has also been found in the chest wall of radiation therapy-treated breast cancer patients [7]. Osteoradionecrosis is often accompanied by osteomyelitis and has a high likelihood of recurrence. The presence of radiation-induced fibrotic tissue is likely to delay wound healing, thereby necessitating extensive surgical resection [4].
This patient had pre-existing conditions of hypertension, diabetes, and chronic kidney disease. Due to fibrosis and calcification in the right lung caused by radiation, pulmonary function was reduced. In the pulmonary function test, the forced expiratory volume in 1 second/forced vital capacity was 67%, indicating moderate obstruction. The left ventricular ejection fraction was 40% on preoperative echocardiography, indicating reduced heart function. The patient’s overall American Society of Anesthesiologists score was 3, indicating a high risk of postoperative cardiopulmonary complications. Therefore, it was necessary to shorten the operation time and minimize the scope of the operation.
Local flaps of various kinds are used for the reconstruction of extensive soft tissue defects in the chest wall. The pectoralis major muscle flap, latissimus dorsi (LD) muscle flap, and vertical or transverse rectus abdominis myocutaneous flaps are the most commonly used. Thoracoabdominal and thoracoepigastric flaps are also sometimes used [8]. The wound in this patient was deep and exposed the pleura, and the pectoralis major muscle was damaged during debridement. The LD flap is advantageous for covering a large wound, but presents the following challenges: changing position during surgery, the use of a major muscle, and frequent formation of seroma at the donor site. The rectus abdominis myocutaneous flap is disadvantageous due to its wider surgical extent and longer operative time than the contralateral breast flap, increasing the risk of postoperative complications, in addition to using a major muscle. In contrast, the contralateral breast flap does not use muscles; therefore, no donor site morbidity can occur due to muscle harvest. This method has a shorter operation time than other perforator-based or free flaps and thus provides advantages for patients at higher risk for general anesthesia-associated complications. Additionally, this method is associated with a shorter recovery after surgery because the surgical extent is limited to the chest area. The patient’s vital signs were stable immediately after surgery, and she was able to resume daily activities, including ambulation, one day after surgery. No donor site morbidity occurred after surgery, except partial dehiscence, which required minor repair.
Reconstruction of the chest wall using a contralateral breast flap should be considered in patients with ptosis or large breasts that can cover the contralateral side, patients with a high risk of postoperative complications due to old age or poor general condition, and patients for whom an LD or rectus abdominis-based flap has already been used or cannot be used.
This technique has two limitations. First, the anatomy of the contralateral breast may be deformed, making breast cancer screening difficult in the future. Second, covering the entire chest with a single breast is not esthetically pleasing.
Nevertheless, the contralateral breast Y-V flap allows simple and quick reconstruction, providing more options for chest wall reconstruction that allow for further alternatives in treatment plans for each patient.