INTRODUCTION
The pedicled or free rectus abdominis myocutaneous flap and the deep inferior epigastric artery perforator (DIEP) flap are commonly used in breast reconstruction with silicone implants. However, previous studies have reported a 5% to 30% rate of necrosis in mastectomy skin and in the nipple-areolar complex following breast reconstruction [1-3]. This complication worsens the aesthetic outcome of breast reconstruction. Because of the nippleŌĆÖs protruding shape, tip or full-thickness necrosis often occurs, making it difficult to reconstruct the original shape [4,5].
In addition to necrosis, there are cases where the nipple must be removed when a subareolar resection biopsy is done to diagnose breast cancer, and reconstruction must be performed. We present a case of successful nipple reconstruction for nipple necrosis that occurred after breast reconstruction using a DIEP flap.
CASE REPORT
A 45-year-old woman was seen in our clinic for left breast cancer. She had undergone reduction mammoplasty 10 years ago, and a vertical reduction scar was observed. A nipple-sparing mastectomy was performed using the previous lower pole incision line and a subsequent DIEP flap reconstruction was performed. Considering the patientŌĆÖs history of reduction mammoplasty, part of the abdominal skin was preserved during surgery without de-epithelialization, in preparation for possible mastectomy skin-flap necrosis.
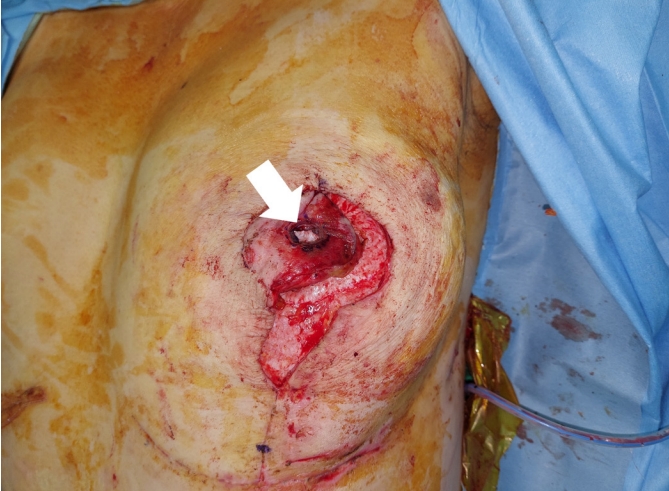
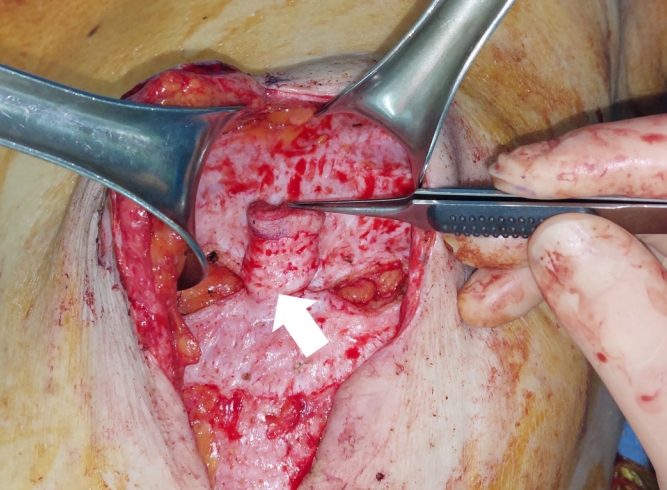
Although there were no immediately identifiable changes in the nipples, the nipple and areolar complex gradually changed color. Twelve days after the surgery, full-thickness nipple necrosis with a conversion to dry gangrene was observed. On postoperative day 15, the necrotized nipple was excised, leaving a soft tissue defect 12 mm in diameter and 15 mm deep (Fig. 1).
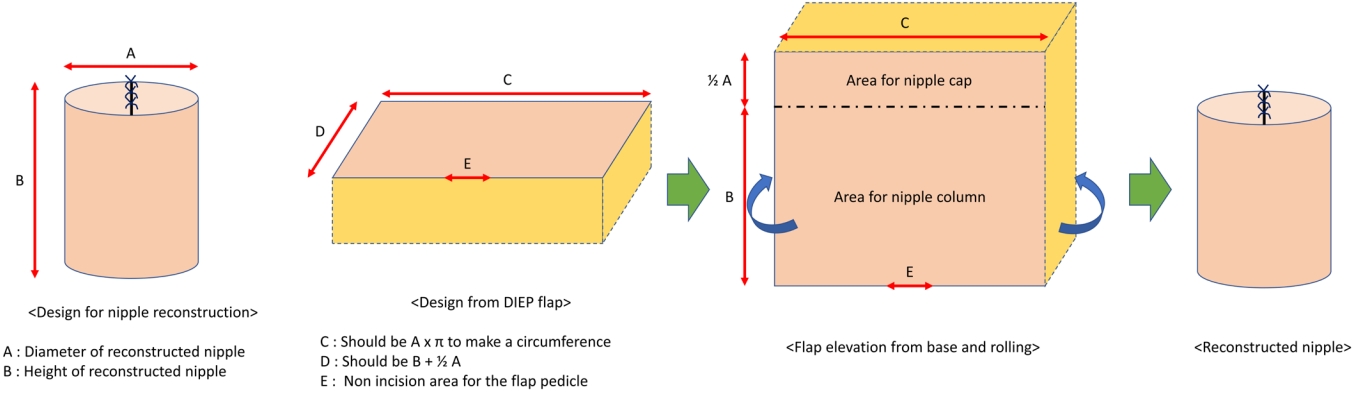
A 38├Ś23 mm rectangular flap was designed from the DIEP flap to cover the defect (Fig. 2). The cylindrical flap was designed with a diameter of 12 mm (12 mm├ŚŽĆŌēł38 mm), and the height of the cylinder was calculated as 23 mm, which was the sum of the mastectomy skin flap thickness (15 mm), nipple projection (2 mm), and half the length of the rectangle (12 mm/2=6 mm) used to make a nipple cap (Fig. 3).
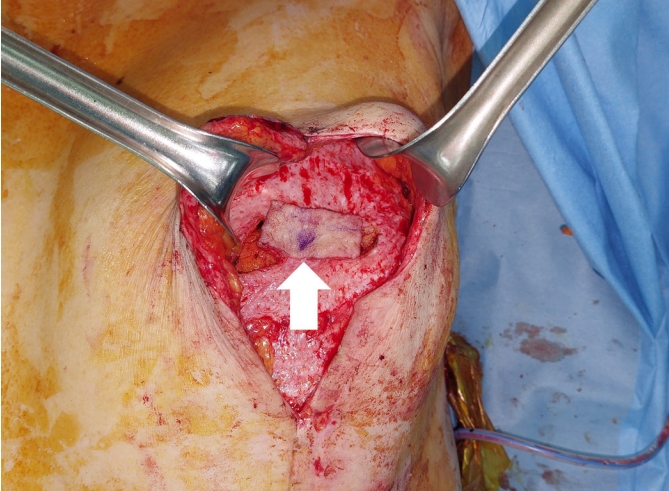
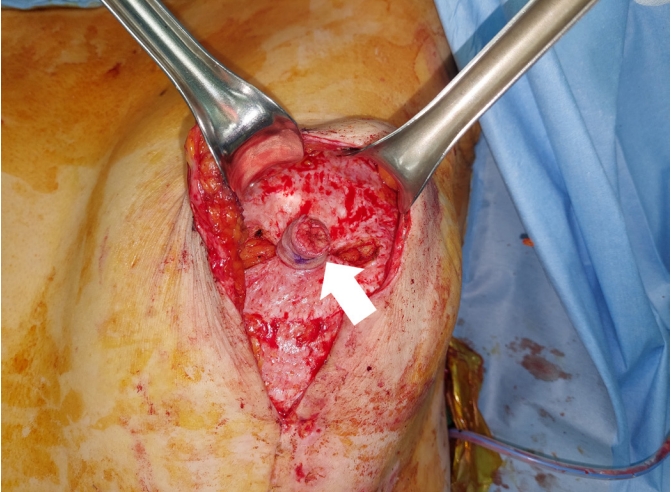
After elevation of the full thickness of the skin and part of the subcutaneous fat, the unexcised middle inferior portion of the rectangular flap measuring 4 mm became a circulation pedicle. After rolling the elevated flap into a cylindrical shape, it was sutured with 4-0 Monosyn (B. Braun, Melsungen, Germany), and the bottom of the cylindrical flap was also approximated between the dermis of the DIEP flap using 4-0 Monosyn; hence, the flap was not depressed (Fig. 4).
After inserting the cylindrical flap into the defect site, the remnant DIEP flap tissue around the nipple-areolar complex was de-epithelialized (Fig. 5). Next, the area between the de-epithelialized site and the mastectomy skin flap and nipple cap was sutured with 4-0 Monosyn. Subsequently, the skin layer was repaired with 5-0 Ethicon (Johnson & Johnson, New Brunswick, NJ, USA) (Fig. 6). The dressing, comprising Terramycin ointment (Pfizer Inc., New York, NY, USA) and non-adhesive foam, was changed daily.
On postoperative day 19, partial skin necrosis was observed on the lateral side of the areola. However, no complications were found on the reconstructed nipple and the projection was maintained (Fig. 7). Although the nipple projection had lost 3 mm by 6 months postoperatively, the patient was satisfied with the result (Fig. 8).
DISCUSSION
Several methods have been introduced to cover postmastectomy nipple necrosis or defects [6-9]. Shestak et al. [10] compared bell flaps, modified star flaps, and skate flaps and reported that the modified flaps yielded the least projection loss. Losken et al. [9] first reported a C-V flap for nipple reconstruction and introduced several modified techniques [6,11,12].
In our case, the thickness of the patientŌĆÖs mastectomy skin flap was 15 mm; thus, there was sufficient tissue from the DIEP flap for nipple reconstruction that reproduced nipple projection. Since the techniques used thus far had resulted in projection loss, a design to minimize the loss was required. Therefore, we formed the rectangular flap into a tall nipple column to avoid depression of the nipple. Although the reconstructed nipple had depressed 3 mm at 6 months, the nipple maintained more than 80% of its initial height (final nipple height from the base: 17 mmŌĆō3 mm=14 mm; initial nipple height from the base: 17 mm; 14/17=82.35%) This degree of projection preservation was significant considering that the previous method only preserved 10.1% to 68.4% of the initial nipple height [13,14]. However, further studies are needed to determine whether these results can be consistently achieved.
Unlike the subcutaneous tissue of the C-V flap, the base of our reconstructed rectangular flap was dermis tissue, which helped avoid projection loss. In addition, the rectangular flap had sufficient vertical length for construction of the nipple cap, which makes the rectangular flap higher than the C-V flap, possibly leading to scar widening at the harvest site or a changed flap shape. However, the abdominal flap tissue, apart from the nipple itself, was placed below the mastectomy skin flap layer, maximizing nipple projection, and thereby avoiding the limitations described above. We believe that the major benefit of our cylindrical design was better flap circulation by providing wider contact of the de-epithelialized area with the mastectomy tissue. This design also resulted in a more natural shape.
Although the abdominal skin was used to reconstruct the nipple and not saved for other possible mastectomy skin-flap necrosis, the small dermal layer that would be needed (i.e., 6├Ś6├ŚŽĆŌēł113.04 mm2 of skin for a nipple cap 12 mm in diameter or 12├Ś9├ŚŽĆŌēł339.12 mm2 of skin for a 9-mm projected nipple column) could heal sufficiently by secondary intention or by a future skin graft using the remnant breast skin.
In conclusion, we suggest that a de-epithelialized rectangular flap would be a good choice for the repair of nipple loss after autologous tissue-based breast reconstruction to maintain the projection of the reconstructed nipple and achieve a better aesthetic outcome.