INTRODUCTION
Hairline correction surgery is an advanced form of hair transplantation and is performed substantially for Korean females with a flat, broad face and prominent zygoma. However, this procedure demands a considerable learning curve in order to acquire natural results because Koreans have coarse hairs and there is a strong contrast in color between their skin and hair color. As a result, quite a few patients are dissatisfied with unnatural results, and consequently secondary hairline correction surgery is required.
Nevertheless, there has not been any study presented yet for secondary hairline correction surgery methods so as to fix unnatural results from primary hairline correction surgery procedures.
Therefore, the author would like to report this matter based on clinical experience and literature review.
METHODS
The author retrospectively reviewed medical records and medical photos of 36 patients who had had secondary hairline correction surgery in my clinic, with long-term followed up from February 2010 to March 2013.
The age of the patients ranged from 20 to 48 years and the average was 30.8 years old. They experienced prior hairline correction surgery 1.4 times on average. All the patients were unsatisfied with the results and visited my clinic. Five of the patients had follicular unit extraction (FUE) and 31 had incisional method hairline surgery in the primary procedure. Six of the patients had hair transplant in slit technique and 31 had in implanter technique. Basically, there was no difference in the pattern of complaints between slit and implanter technique. However, the complaints about slit technique were mainly the unnatural directions of hairs. It seems that the problem occurred because in procedure surgeons only did slit creations and let nurses or technicians do a graft placement. For the rest of the complaints, no significant differences were reported between slit and implanter technique and it shows that surgeonsŌĆÖ proficiency is more important than types of surgery (Table 1).
It took 2.8 years on average for the patients to have secondary hairline correction surgery. One of the patients, with the most surgery experience, had hairline correction surgery 5 times in 3 different clinics, but was still unsatisfied with the unnatural results in appearance.
The total number of the patients was 36. For 20 patients, new anterior hairline forward the previous one was created. 6 patients had FUE punch extraction for wrongly implanted hairs at the anterior hairline and new hairline was created for them by secondary hiar implantation.
Six patients had secondary hair transplantation after laser hair removal treatment on previously implanted hairs. Intense pulsed light (IPL) was used for laser hair removal and 3-5 times of the treatment were carried out with the average 2-month interval. And then, secondary hairline correction surgery was performed after waiting for 3-6 months to confirm no more hairs were growing on the recipient sites.
Four patients initially had punch extraction for some of the hairs implanted on the previous frontal hairline. New hairline creation was performed after the recipient sites became soft while wounds were healing (Table 2).
Donor scar widening was seen in 4 patients, so additional hair harvest and donor scar revision were simultaneously conducted.
The average amount of implant procedure was 1,260 grafts and 2,230 hairs.
RESULTS
All the results were satisfactory. The average period of a follow-up was 11.6 months, ranging from 6 to 37 months. 3 out of total 36 patients (8.3%) had touch-up procedure.
All 3 cases of touch-up were for intensifying hair density. The implanted amount for intensifying density was from 86 to 460 hairs, with an average of 286 hairs. All the patients were pleased with the retouching results.
Mild folliculitis was seen on the recipient site in 1 case, but it was improved simply after potadine dressing and antibiotics medication.
No specific adverse reactions occurred.
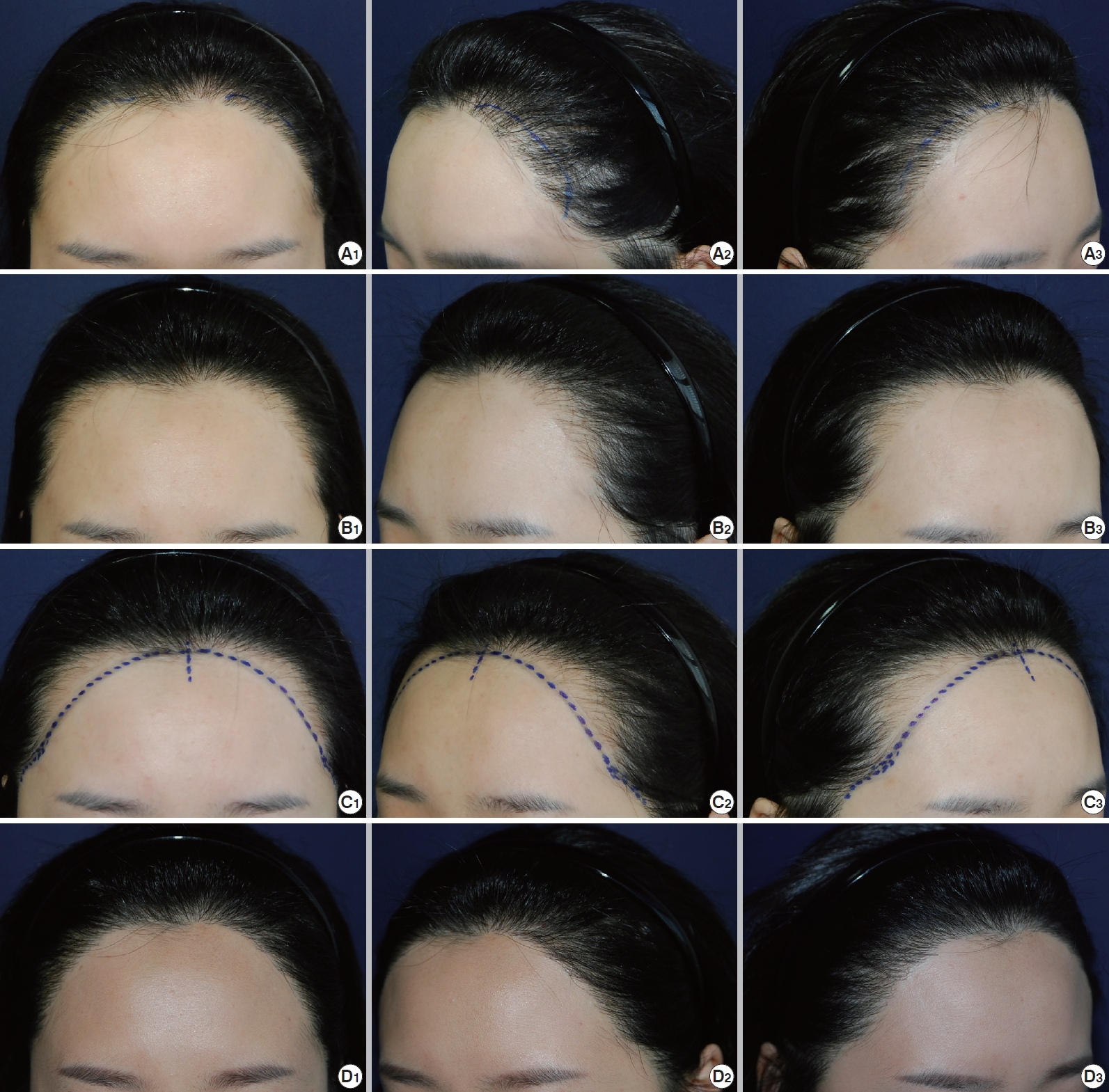
Case 1
Twenty-eight-year old woman after previous twice of hairline correction surgeries, she visited us for complaints of low density, improper hair angle and direction and unnatural appearance. Five times of laser hair removal of previously placed grafts was done first, and recreation of new hairline was done 3 months after the last session of laser hair removal (Fig. 1).
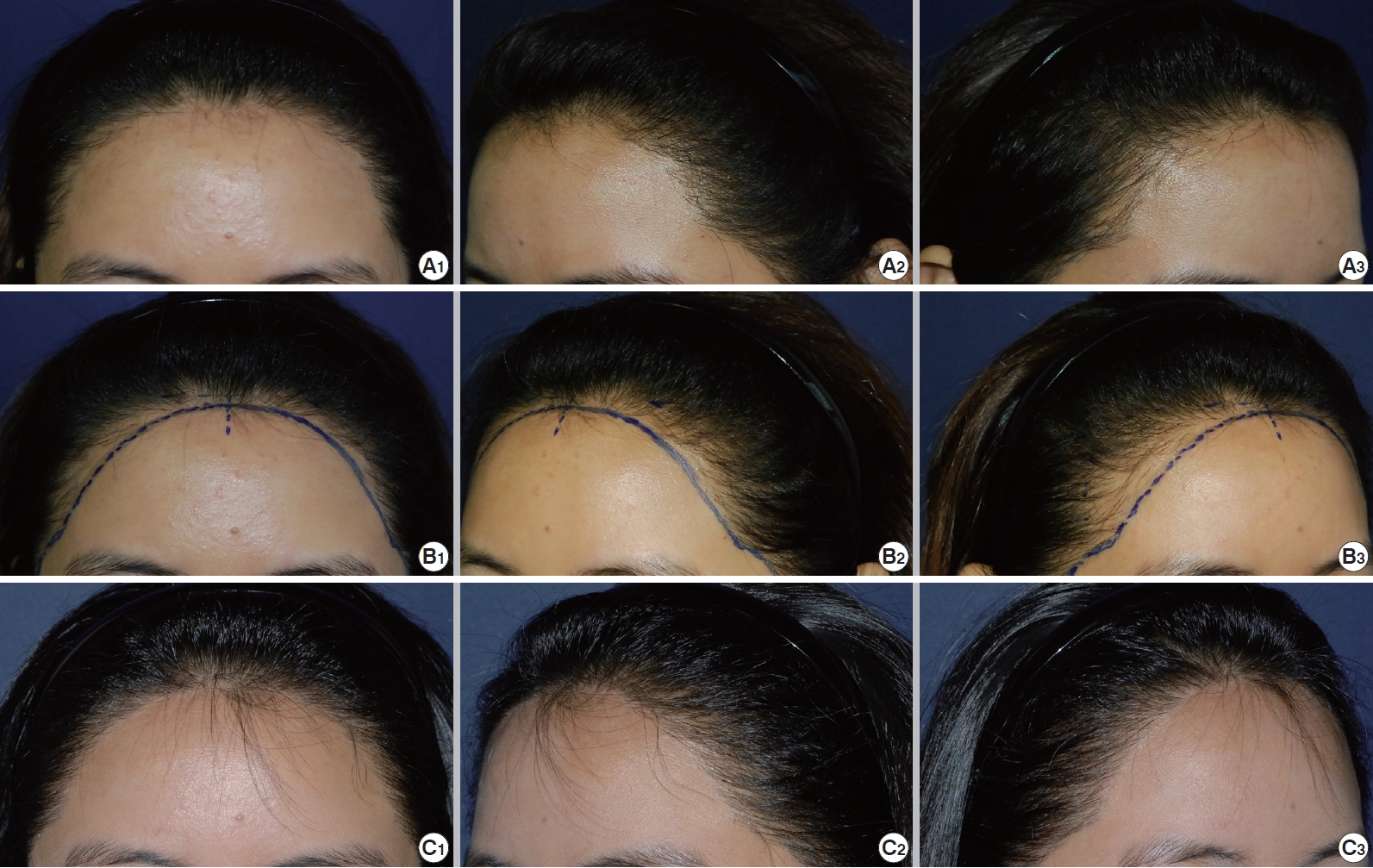
Case 2
Twenty-four-year old woman visited the clinic due to unnatural appearance after hairline correction surgery at other clinic. In order to enhance low density and unnatural hair direction seen, natural new hairline for camouflage was created in the manner of fencing up in front of the pre-existing hairline (Fig. 2).
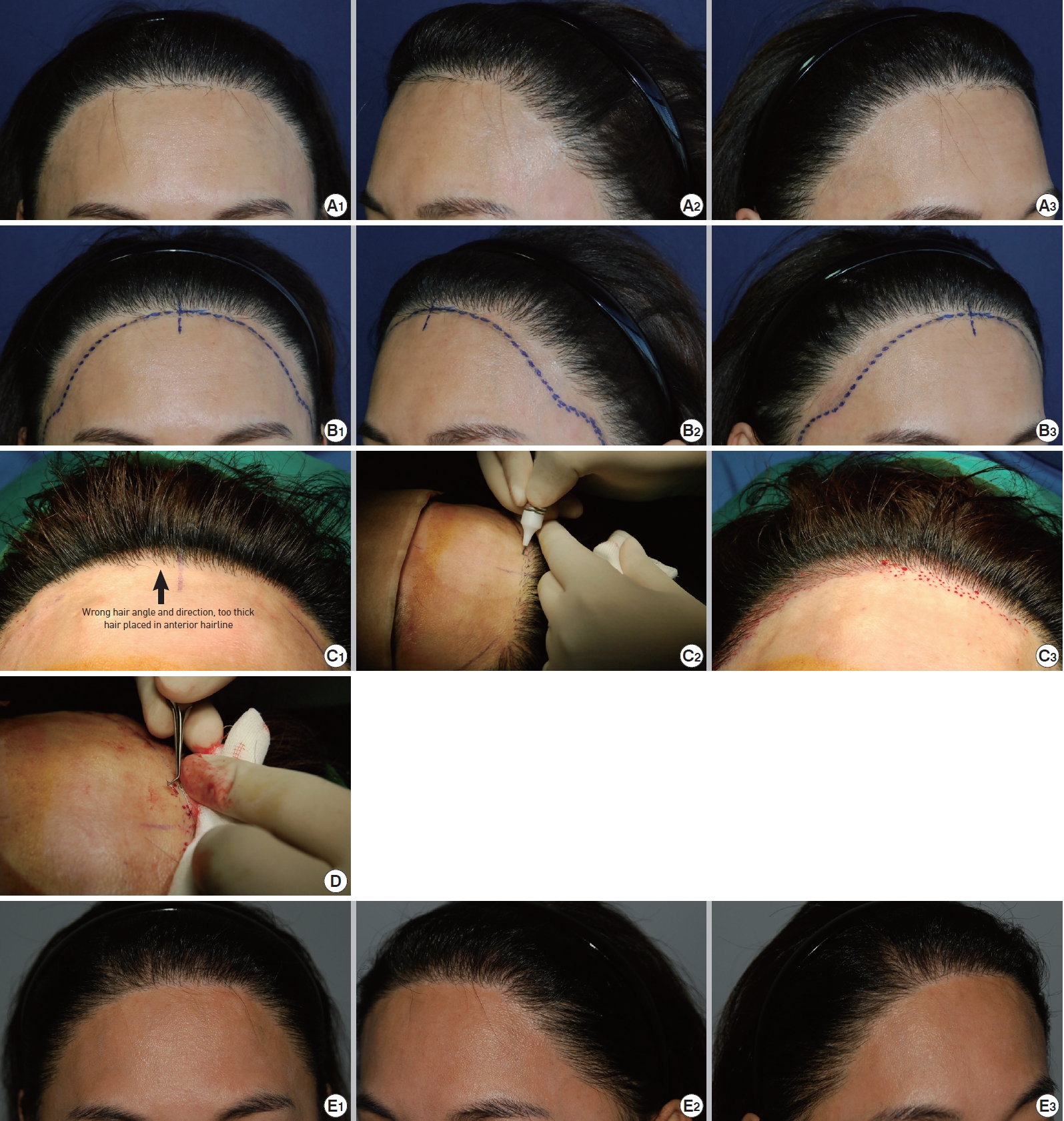
Case 3
Thirty-five-year old woman had 3 times of hairline correction surgery at other clinic resulting in unnatural appearance due to wrong hair angle and direction, too thick hair placed in anterior hairline, severe scarring on recipient site and low density (Fig. 3).
The unnaturally looking hairs growing at frontal hairline area were removed by FUE technique and new hairline has been made and transplanted (Fig. 3).
Case 4
Forty-five-year old woman had hairline correction surgery resulting in unnatural appearance. She had 4 times of additional secondary correction surgeries at 3 different clinics, but there were still problems such as improperly matched hair curliness, low density, wrong hair angle and direction, severe scarring on recipient site and unnatural appearance. New hairline was created to camouflage and hide the pre-existing hairline with simultaneous FUE removal of some improperly placed hairs (Fig. 4).
DISCUSSION
From the late 1990s, the concept of follicular unit transplantation was established [1]. Ever since, the hair transplantation field has accomplished a remarkable development. In 2002, follicular unit extraction was introduced by Rassman and Bernstein. In the mid2000s, the trichophytic closure method was presented [2-4]. Hair transplantation surgery is not only regarded for reconstruction purposes but also adopted in the aesthetic surgery field, widely performed in Korea with the name of hairline correction surgery.
Forehead reduction used to be the sole solution for a wide forehead. With surgical skill development, however, hair transplantation also became a way to naturally fix a wide forehead [5,6]. Jung et al. [7] introduced the classification of basic hairline shapes for Asian females and foundational surgery methods. Park [8] suggested that hairline correction surgery can camouflage the remaining posterior zygomatic arch protrusion when there is no clear improvement even after zygoma reduction surgery. Bertram [9] has presented his personal experience of female hairline advancement in Chinese females. No secondary correction methods, though, has been suggested in literature when unnatural results have arisen in hairline correction surgery.
The following are the major complaints from patients and methods for improving procedures (Table 3). The correction methods listed in Table 3 must be chosen case by case. Perhaps it is required for surgeons to have many years of surgical experience.
There are several precautions in secondary hairline correction surgery. First, serious scarring on the recipient site is frequently seen, assumedly due to traumatic manipulation in the primary surgery. In this case, a high level of attention is needed in preparation for low survival, excessive popping or bleeding in procedure. It is desirable to explain to patients in advance the related information and the possibility of a retouch procedure for intensifying density.
Second, accurate donor evaluation is necessary. Scalp laxity in the occipital region may not be enough for secondary procedure. Therefore, donor scalp laxity and density must be checked in the advance consultation. Otherwise, it can lead to problematic situations on the day of the surgery.
Third, for secondary correction surgery, it is preferable to wait more than three months after laser hair removal and to check the possibility of hair regrowth on the recipient site.
Fourth, in punch extraction, a punch size of 0.8 mm diameter or less must be used in order to avoid hypopigmented dot scar on the extraction site. From authorŌĆÖs experience, a 0.8 mm punch is recommended because it didnŌĆÖt make any visible scars. In the process of punch extraction, along with the direction of hairs seen outside the skin, scoring punching is performed using a sharp punch just until 2-3 mm in depth, and then forceful grip and extraction is practiced with forceps. In case of punch extraction does not work well in the manner described above, additional 1-2 mm can be tried with care.
Fifth, for too thick hairs, it is worth considering single hair graft by splitting into single hairs.
Sixth, too deep or crooked follicles previously implanted are occasionally seen due to improper placement techniques. In this case, punch extraction is not a simple task. Thus, without a high degree of attention, serious folliculitis can be caused by pushing follicles into a deeper depth.
Seventh, it is recommend to make an acute angle in hairline. In general, following the same direction of pre-existing hairs results in natural appearance. For the most significant indicator in hair transplant is pre-existing hair contiguous to the recipient sites.
Eighth, considering side hairline, creating temporal peaks is essential to complete natural appearance. Regarding mid-frontal hairline, the mid-frontal height can be naturally lowered to the extent of about 1cm. Around 3-4 natural peaks should be created in the zigzag pattern in each side. Also, it is desirable to create a widowŌĆÖs peak as 1.5 times larger as the peaks on each sides.
If secondary hairline correction surgery is performed with an awareness of the precautions mentioned above, satisfactory procedure results are anticipated.