INTRODUCTION
There are a number of types of rhinoplasty techniques. It is clear that the open rhinoplasty approach has advantages in treating complex and difficult nasal deformities, because it allows a great range of nasal structures to be directly viewed. However, a transcolumellar incision may be troublesome [1]. The closed approach appears to be especially useful for simple nasal surgery. The surgeon’s experience and sense of aesthetics are essential for the closed approach, because the operation is performed without exposing the nasal structures [2]. An intraoral approach can be used by anyone who wishes to avoid a nasal scar. Through an intraoral approach, surgeons can insert grafts or implants easily [3]. Surgeons must choose the appropriate approach that provides patients with the best aesthetic results.
We present our experience with calvarial bone framework insertion through an intraoral approach in a patient who had columellar scar contracture after open rhinoplasty.
CASE REPORT
A 58-year-old woman who had undergone rhinoplasty visited our hospital. The augmentation rhinoplasty had been carried out using Goretex® (W.L. Gore & Associates Inc., Flagstaff, AZ, USA) through the open rhinoplasty approach. The premaxillary area was also augmented using Goretex® through an intraoral approach. After several years, the implants had become distorted and displaced, causing pain and tenderness. The patient showed severe columellar scar contracture accompanied with an over-elevated nasal dorsum, short nose deformity, and turned-up nose.
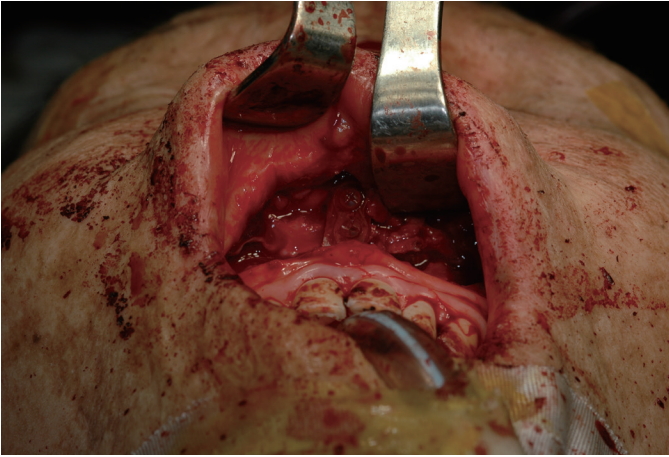
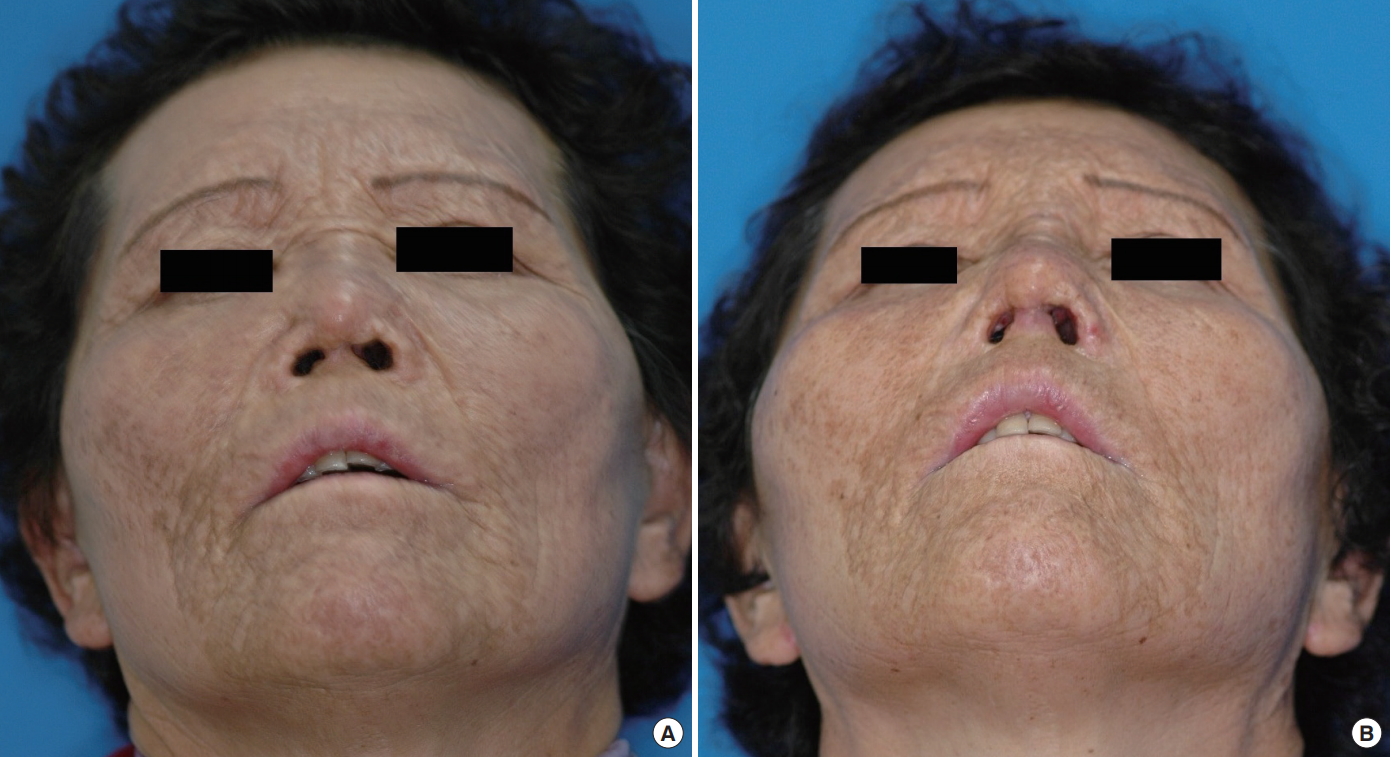
The patient wanted to remove the Goretex® on the nasal dorsum and premaxillary area due to the discomfort. At the same time, she did not want to worsen her appearance. With the patient’s consent, the nasal implant was removed after bilateral rim incision, and the implant in the premaxillary area was removed through a gingivobuccal incision under general anesthesia (Fig. 1). However, severe columellar scar contracture was present and the surrounding tissue was fragile. The columellar tissue was too vulnerable to be touched. We were not able to incise the columella or insert new nasal implants through bilateral rim incisions. Moreover, the patient had septal cartilage perforation and collapse. The patient required columellar support as well as nasal dorsum reconstruction. We performed an autogenous L-strut bone framework graft through an intraoral approach. Two pieces of 5 cm×1 cm split calvarial bone were harvested and trimmed to fit the width and length of the nasal dorsum and columella. The right-angle-shaped bone framework was formed with an absorbable plates and screws (Fig. 2). Through a gingivobuccal incision, the tissue was spread open widely. After the bone framework graft insertion, the caudal part of the bone framework was fixed at the anterior nasal spine of the maxilla using an absorbable plate and screws (Fig. 3). We confirmed that it was solidly fixed (Fig. 4). The wound was closed without any problems. The patient did not experience any complications, such as columellar necrosis or graft inflammation. A photograph taken 8 months after the operation shows a lengthened columella and good nasal tip projection (Fig. 5 and 6). The patient was satisfied with the outcome.
DISCUSSION
Multiple autogenous and alloplastic implants are used for augmentation rhinoplasty and the reconstruction of nasal deformities. Autogenous implants include auricular and septal cartilage grafts as well as rib bone and iliac crest bone grafts. Alloplastic materials include acrylic, supramid mesh, Goretex®, and silicone rubber. Autogenous grafts have been shown to provide excellent, long-term, reliable results in nasal reconstruction [4]. Autologous and homologous cartilages have proven to be more efficient in the correction of minor deficiencies of the columella, nasal dorsum, and nasal tip. However, these are inadequate for major bony defects that require structural reconstruction due to the limited size of the cartilage, unpredictable resorption rates, and their inability to achieve fixation to the underlying bone [5].
Autogenous calvarial grafts were used in the 1890s as part of an osteocutaneous flap by König and Müller. In 1983, Jackson et al. [6] reported their experience with autogenous calvarial grafts in nasal reconstruction. Calvarial grafts can be harvested easily. Moreover, the scar is often unnoticeable because it is covered with hair. The donor site is not painful compared with other bone graft donor sites. In addition, recent studies have indicated that calvarial bone grafts have better survival rates than nonmembranous bone grafts obtained from other donor sites [7]. The risk of intracranial injury during harvesting has been mentioned, but clinical reports are rare.
Recent studies have addressed the importance of rigid fixation for primary bone healing with decreased absorption. When onlayed autogenous bone grafts are rigidly fixed, improved results can be expected with respect to graft resorption, regardless of the type of bone utilized (membranous versus endochondral). The experimentally proven advantages of rigid fixation include primary bone healing and reduced bone resorption [8]. Other studies have shown that craniofacial bone healing using absorbable fixation systems offers results similar to those of metallic fixation systems, with lower rates of complications [9]. Once grafts became adherent enough to the recipient site to resist external mechanical forces, the type of fixation employed makes no difference. In our surgery, the surface of the bone framework was not completely in contact with the normal periosteum and bone. Therefore, a higher resorption rate is expected than has been observed in recent research. Nevertheless, we used a bone framework because it provides a strong supporting force and will act as a scaffold for a certain time.
In this case, we chose an intraoral approach because the patient had severe scar contracture of the columella and the adjacent tissues were too vulnerable to make a transcolumellar incision. Through the intraoral incision, we were not only able to sufficiently expose the previously grafted material, but were also able to prevent further scar contracture of the columella and easily fix the bony framework to the anterior nasal spine. However, the depressor septi nasi muscle could be damaged when using an intraoral approach. During the short-nose correction, the contracted soft tissue had to be sufficiently released and the autologous grafts had to provide mechanical support to prevent relapse. Furthermore, over-dissection of nasal soft tissue could result in contracture that would worsen the short-nose deformity.
To our knowledge, nasal grafting using an intraoral approach in patients with columellar scar contracture has rarely been reported. Our experience is meaningful because this patient underwent nasal grafting with a calvarial bone framework, using an absorbable plate and screws through an intraoral approach.
We confirmed the realistic possibility and good aesthetic results of bone framework grafting through an intraoral approach in a patient who had scar contractures in the columella, septal cartilage perforation, and collapse.