INTRODUCTION
Lipoma is a benign mesenchymal tumor and the most common soft tissue tumor [1]. Giant intramuscular lipomas are deep-seated within the muscle [2], and are defined by a measurement greater than 10 cm in any dimension [3]. Most patients with a giant lipoma desire surgical excision for esthetic reasons, and others want surgical resection because of pain secondary to compression or expansion of an adjacent peripheral nerve [4,5].
Traditionally, a long surgical incision has been necessary for total excision of a deep and large intramuscular lipoma, resulting in a long scar and esthetic dissatisfaction. Reducing the scar length by shortening the incision results in tissue injury around the incision margin from traction, which may hinder healing and lead to the formation of hypertrophic scars [6,7].
Some other methods have been suggested to shorten the scar, including suction-assisted surgical excision, endoscopic-assisted liposuction, and endoscopic excision for removing moderate and large lipomas [8-10]. However, it is difficult to achieve complete removal of a lipoma and its entire capsule with these methods, and their recurrence rate has been reported to be high [11].
The present study suggests that using an ultrasonic energy device minimizes the scar after excision of a giant intramuscular lipoma.
CASE REPORT
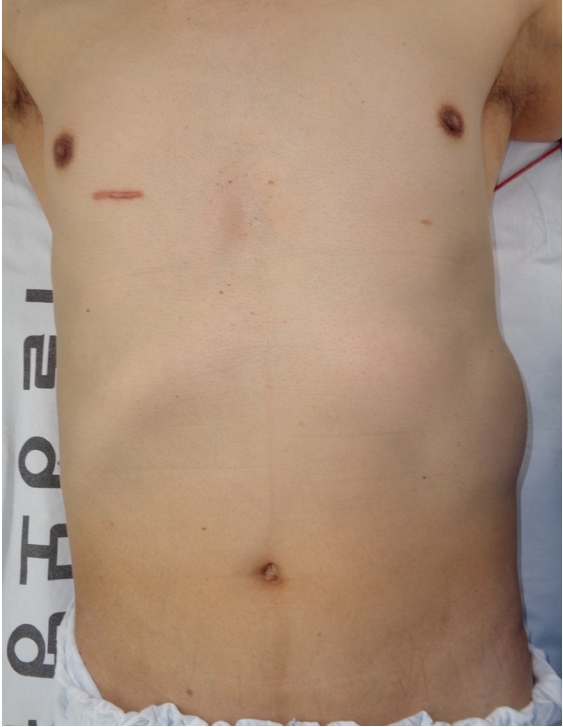
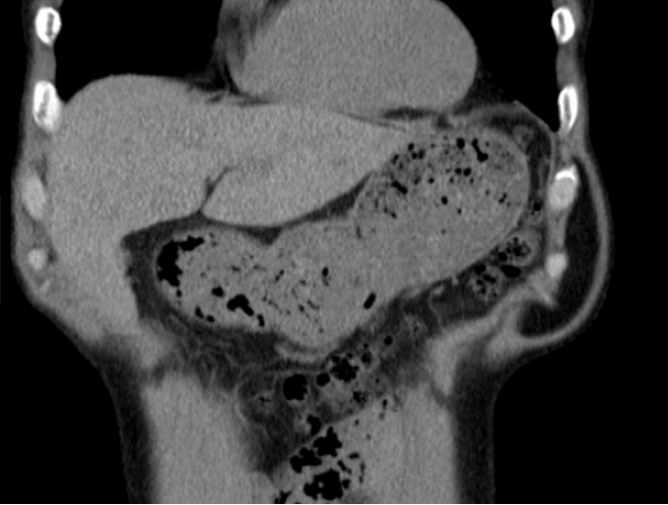
A 62-year-old male patient was admitted with a giant intramuscular lipoma located in his anterolateral abdominal wall (Fig. 1). The patient desired complete removal of the lipoma for diagnostic and cosmetic purposes, but he was concerned about postoperative scarring because he had the tendency to form hypertrophic scars, as seen on his right chest (Fig. 1). Computed tomography (CT) revealed a lipoma measuring 10Ă10 cm located deep in the external oblique muscle (Fig. 2). Although a benign lipoma was suspected, CT did not completely exclude the possibility of liposarcoma.
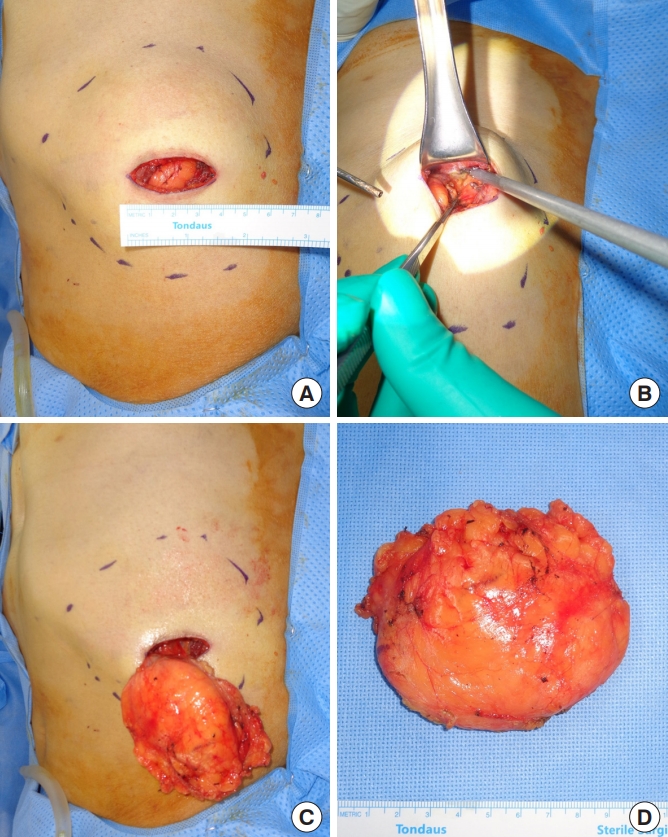
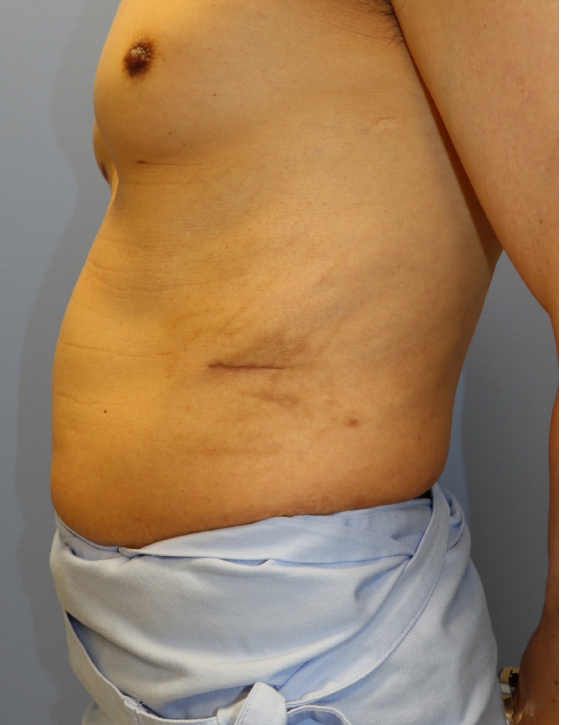
With the patient under general endotracheal anesthesia, surgical excision was performed. The skin incision was only 3.5 cm long. After dissection of the subcutaneous layer, the muscle was split to expose the lipoma (Fig. 3A). A mass, seated under the muscle layer, was completely removed using a harmonic scalpel (Harmonic HD; Ethicon, Somerville, NJ, USA). A strong traction force was not required to secure the operative field of view in this procedure (Fig. 3B-D). The entire operation took 40 minutes. The ultrasonic harmonic scalpel simultaneously accomplished hemostasis and dissection, and although the operation time was reduced, the dissection was performed meticulously. No perioperative complications were noted. Postoperatively, the patient was esthetically satisfied with the 3.5-cm-long scar (Figs. 4, 5).
DISCUSSION
Lipoma is a benign tumor originating from the mesenchyme, and it is the most frequent type of soft tissue tumor [1]. Giant intramuscular lipomas are deep-seated lipomas that measure greater than 10 cm in any dimension [3], and an extended incision length may be necessary to achieve complete resection of the lipoma and its entire capsule. In this report, an ultrasonic harmonic scalpel was used to ensure full visualization of the operation field and easily remove a 10Ă10-cm giant intramuscular lipoma with a minimal incision length.
In the traditional excision procedure, utilizing a small incision to shorten the postoperative scar requires a high traction force to obtain the appropriate visual field; as a result, tissue and incision margin injury might occur, leading to poor wound healing or hypertrophic scar formation [6,7].
In contrast, the ultrasonic harmonic scalpel is a surgical instrument frequently used in laparoscopic surgery that provides an appropriate field of view for the operation with small incisions and without the requirement of a strong force of traction. Minimizing mechanical forces in the wound environment improves wound healing and reduces scar formation [6].
The ultrasonic harmonic scalpel can simultaneously perform cutting and cauterization. Thus, it can be used to perform a meticulous operation and to shorten the operation time. Moreover, the lateral thermal spread of the harmonic scalpel is minimal, so it may be helpful for minimizing thermal damage around the tissue [12].
Moreover, using the harmonic scalpel reduces the occurrence of seroma, because the ultrasound energy of the device prevents the opening through which serous discharge occurs. However, dissection with this energy-delivering device in a narrow field is predicated on sufficient anatomical knowledge. By ensuring a thorough understanding of the blood vessels and nerves to be dissected in the region of the lipoma, intraoperative bleeding can be minimized and the sequelae after surgery can be reduced.
Various surgical techniques that improve esthetic outcomes by shortening scar length have been reported, including suction-assisted surgical excision, endoscopic-assisted liposuction, and endoscopic excision for removing moderate and large lipomas [8-10]. Liposuction is one of the most helpful options for removing large, diffuse-spreading, and ill-defined suprafascial lipomas [13]. The advantages of liposuction include smaller scars, less pain, cost-effectiveness, reduced operative time, lower complication rates, and a better final contour [11]. However, the lipoma tissue is fragmented in the process of liposuction, and it is difficult to perform an accurate pathological analysis. Therefore, a preoperative fine needle aspiration biopsy or magnetic resonance imaging should be considered in patients with a questionable mass [14]. Moreover, a higher recurrence risk due to tissue fragmentation has been reported [11,15].
Compared with the previously reported methods, the ultrasonic harmonic scalpel has a lower recurrence rate and has the advantage of permitting lipoma excision en bloc, even in large and deep-seated lipomas, so that pathologic specimens can be precisely analyzed.