Cocktail therapy including bleomycin and verapamil as a promising treatment choice for keloid scars
Article information

Abstract
Background
The treatment of keloids is both challenging and controversial. Until now, there is no definitive treatment modality for keloids. To determine the efficacy and safety of an intralesional cocktail therapy, including bleomycin compared to corticosteroid injection method on the treatment of keloid scars.
Methods
A retrospective chart review was performed for 35 patients diagnosed with keloids. The cocktail therapy regimen consisted of bleomycin, 1% lidocaine, verapamil, and triamcinolone, which was further diluted with 1 mL of normal saline. In group B, 1mL of triamcinolone acetonide was injected into the lesion. Results for a total of 35 patients included in this study were evaluated according to their therapeutic responses and complications six months after the last session.
Results
Analyzing the outcomes of the patients treated with a cocktail regimen (group A), it was found that 87% showed favorable therapeutic responses (scar thickness <50%). In group B, 58% of patients showed favorable therapeutic responses. No major complications were observed in both groups.
Conclusions
High therapeutic response rates without major complications were identified in this study, suggesting that cocktail therapy with bleomycin can be considered a safe and effective treatment modality for keloid scars.
INTRODUCTION
Scarring causes severe psychological and aesthetic stress for patients, reducing their quality of life. The pathogenesis of keloid scars is not fully understood. According to current research, keloid scars arise from mechanical force, infection, or other factors, such as a genetic predisposition [1]. However, researchers are still working to understand the exact mechanisms of keloid formation. Consequentially, the treatment of keloids is both challenging and controversial. Until recently, treatment modalities have included surgery, intralesional steroids, compression silicone gel sheets, and radiotherapy, as well as more experimental therapies such as interferons, bleomycin, and 5-fluorouracil (5-FU) [2-6]. Although these trials have shown some promising results, there is no definitive treatment modality for keloids. In this study, we investigated the efficacy and safety of an intralesional cocktail therapy including bleomycin and verapamil compared to corticosteroid injections for the treatment of keloid scars.
METHODS
In this study, a retrospective chart review was performed of 35 patients diagnosed with keloids between August 2016 and July 2019. Patients who were treated with only surgical excision, cocktail therapy after surgical excision, and tranilast (an antiallergic drug), as well as patients lost to follow-up within the first 3 months, were excluded from the study. Twenty-three patients were treated with a cocktail therapy regimen (group A) and 12 patients were treated with intralesional triamcinolone (group B) (Tables 1, 2).

Characteristics of keloid patients treated with cocktail therapy
The cocktail therapy regimen consisted of 0.1 mL of bleomycin (bleomycin HCl, 15 mg), diluted in 20 mL of 0.9% normal saline, 0.3 mL of 1% lidocaine, 0.1 mL of verapamil (verapamil HCl, 5 mg/ 2 mL), and 0.4 mL of triamcinolone (triamcinolone acetonide, 40 mg), which was further diluted with 1 mL of normal saline. In group B, 1 mL of triamcinolone acetonide (40 mg/mL) was injected into the lesion (Fig. 1). In both groups, the applied dose was 1 mL/cm2 of skin. A 30-gauge needle was used to help minimize pain. Sessions were held 1 month apart, and outcomes were analyzed at 1 month after four sessions were completed.
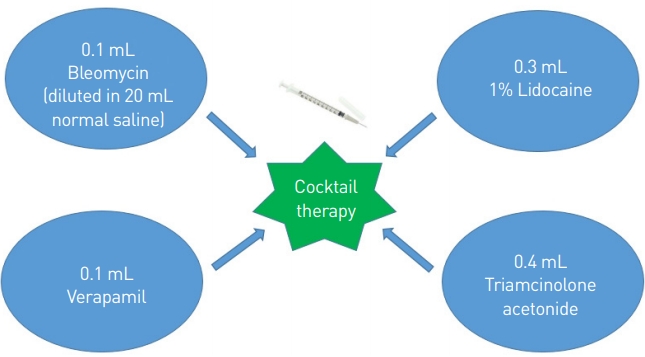
Schema of cocktail therapy regimen for keloid patients.
Intralesional treatment (groups A and B) was indicated for keloids that could not be eliminated by excision, or which had recurred after excision, as well as for keloids ineligible for radiotherapy. This modality was not applied in infected scars. Furthermore, patients with hypersensitivity, allergies to the cocktail components (bleomycin, triamcinolone, and verapamil), or open wounds were excluded from therapy.
The results for the 35 patients who underwent intralesional treatment were evaluated according to their therapeutic responses and complications. When evaluating outcomes, a >50% reduction of scar thickness was considered to indicate a therapeutic response, while recurrence was defined as increased thickness. In addition, three blind observers who specialized in plastic surgery assessed the patients’ photographs using the Vancouver Scar Scale (VSS). The change in the mean score (before treatment–after treatment) in each group was recorded. After data collection, the t-test was conducted for statistical analysis. Complications were defined by the occurrence of ulcers, pain, hyperpigmentation, or hypopigmentation.
RESULTS
In total, 35 patients were treated for keloid scars. Group A, in which cocktail therapy was used, comprised of 23 patients (12 males and 11 females). Group B comprised of 12 patients (five males and seven females). The most common etiology in both groups was previous surgery, followed by vaccination and piercing. Analyzing the outcomes of the 23 patients treated with the cocktail regimen (group A), it was found that 87% of the patients (20/23) showed a favorable therapeutic response (scar thickness <50%). In group B, 58% of the patients (7/12) showed a favorable therapeutic response (Table 3, Figs. 2, 3). The t-test indicated a superior therapeutic response in group A (P<0.05), in which patients were treated with the cocktail regimen. The mean VSS difference was 3.74 in group A and 2.13 in group B, which was statistically significant (P<0.05). Recurrence was not noted during the 6-month follow-up period in group A, but two cases emerged in group B (17%). Pruritis was relieved completely in 17 patients (74%) in group A and in nine patients (75%) in group B. No major complications were observed in either group.

Therapeutic outcomes of cocktail therapy and triamcinolone in keloid patients
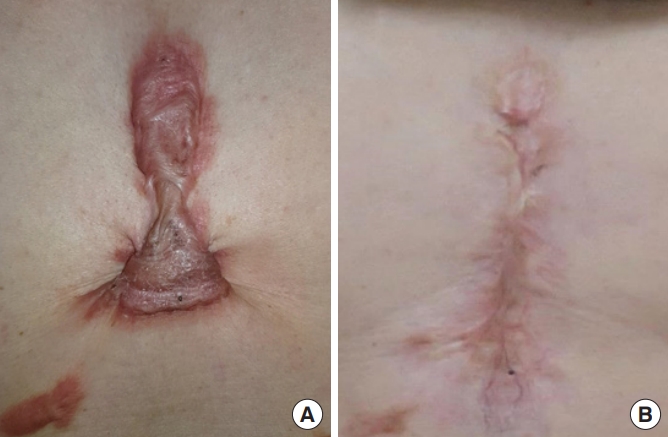
(A) Keloid on the anterior chest of patient 15 (cocktail therapy). (B) Complete flattening after 4 sessions of cocktail regimen. There was no recurrence in 20 months.

(A) Ulcer occurred on the right shoulder of patient 12 (cocktail therapy) after 4 sessions. (B) Complete healing after 3 weeks of conservative dressing with antibiotic ointment.
The minor complications in group A presented as deep ulcers (30%), pain (26%), and hyperpigmentation (57%). Most deep ulcerations healed within a few weeks, and the onset of pain began after injection but dissipated within 5 to 7 days. Hyperpigmentation was identified a few weeks after completion of the final session, but gradually resolved during the 6-month follow-up period. The most common complications in group B were hypopigmentation (42%) and pain (33%).
DISCUSSION
Keloids cause both psychological and aesthetic stress in those afflicted. As the pathogenesis of keloid scars is not fully understood, there is no gold-standard treatment and numerous clinical trials are regularly initiated to address this unsolved problem.
Recently, antineoplastic agents have been shown to improve the treatment response rate, to reduce the recurrence rate, and to minimize the symptoms of scars [7]. Considering the anti-tumoral characteristics of these agents, several trials have shown favorable results when they were used alone or in combination with traditional treatments, such as corticosteroids.
Triamcinolone acetonide is the most widely used intralesional injection component in the treatment of keloid scars, and it is known to inhibit the growth of fibroblasts and transforming growth factor-beta 1, while promoting collagen degradation [8]. Gupta and Kalra [4] treated keloids with 5-FU weekly, finding that ~50% of patients showed a therapeutic response. Khalid [9] injected 5-FU in combination with triamcinolone acetonide, and the effectiveness of the combined treatment was significantly better than that of triamcinolone acetonide alone (77% vs. 49%). Similarly, several trials have investigated various therapies in combination with 5-FU, such as corticosteroids and pulsed dye laser. Because of the generally favorable effects, combination therapy is considered to be more acceptable to patients and physicians [10,11].
Bleomycin is a novel antineoplastic agent known for its efficacy in keloid treatment. Isolated from Streptomyces verticillus, it is primarily used in certain malignancies, such as squamous cell carcinoma, testicular cancer, and Hodgkin disease. As a cytotoxic polypeptide with anti-tumoral properties, bleomycin is known to cause dyskeratosis to the structure of the skin. In a previous study by Templeton et al. [12], dyskeratosis was observed after injecting bleomycin into the subdermal layer of normal human skin. Necrosis of the epidermis, sub-epidermal bullae formation, and dense neutrophilic infiltrates were identified by histologic analysis. In addition, bleomycin is known to inhibit collagen synthesis in fibroblasts. According to Hendricks et al. [13], incubating skin fibroblasts with bleomycin resulted in significant dose-dependent inhibition of DNA synthesis. These characteristics of bleomycin have led to clinical trials in keloid treatment.
There have been several trials of bleomycin for keloids (Table 4). Espana et al. [14] treated keloids and hypertrophic scars by intralesional bleomycin infiltration using multiple needle punctures. In the 13 patients, more than a 90% therapeutic response was seen after one to five sessions. Bodokh and Brun [15] showed a total regression of 84% in 31 keloids and five hypertrophic scars, using intralesional infiltration of bleomycin. Naeini et al. [16] reported 88.3% resolution using bleomycin tattooing, although hyperpigmentation was observed in 75% of patients. Furthermore, Khan et al. [17] reported better Patient and Observer Scar Assessment Scale (POSAS) scores in patients treated with intralesional bleomycin than in those treated with intralesional triamcinolone acetonide.

Previous studies using bleomycin or verapamil as a treatment modality for keloids
Verapamil, a calcium channel blocker that is commonly used for the management of hypertension and arrhythmias, also reduces extracellular matrix production and induces fibroblast procollagenase synthesis. In addition, verapamil inhibits interleukin-6 and vascular endothelial growth factor production by augmenting the expression of decorin [18]. Since triamcinolone decreases the activity of proteinase inhibitors, and verapamil plays a role in increasing the activity of proteinase inhibitors, combining the two drugs increases collagenase levels, which ultimately leads to collagen degradation in the scar [19]. Kant et al. [20] evaluated 58 patients treated with a 1:1 mixture of triamcinolone (40 mg/mL) and verapamil (2.5 mg/mL). In his study, significant improvements in scar surface area, symptoms, and POSAS ratings were observed. These results, combined with therapy, brought about the idea of a cocktail therapy composed of bleomycin, triamcinolone acetonide, and verapamil.
The results of this study demonstrate the potential of a high therapeutic response in treating keloids without major complications such as stroke, anaphylaxis, or pulmonary fibrosis. Although we classified ulcers as a complication and the rate was relatively high (30%), it was lower than the ulcer rate in Saray’s study, according to which all scars treated with bleomycin developed ulcers and crusts at the injection site [21]. Through appropriate pain and infection management, however, the ulcers were temporary and healed without additional complications.
To the best of our knowledge, this is the first clinical trial to describe the efficacy of bleomycin combined with triamcinolone and verapamil for the treatment of keloids. However, there are several limitations of this study. Most importantly, the sample size was relatively small and there were considerable differences between groups. As keloids have a relatively low incidence (0.9% to 1.5%) in Asia [22] and patients with hypertrophic scars were excluded from the study, the number of keloid patients was inevitably limited. In this situation, our focus was on identifying the therapeutic efficacy and safety of our new cocktail therapy in keloid patients. In addition, the primary mechanism and interactions of the agents in this cocktail therapy (bleomycin, triamcinolone, and verapamil) could not be identified. Nonetheless, we observed a favorable therapeutic response without major complications, even in problematic keloid scars. More placebo-controlled studies are needed to elucidate the interactions of the drugs included in the cocktail regimen. Additionally, more precise and objective scar evaluation systems including the POSAS and VSS should be used in the future.
In conclusion, there are several options for keloid treatment, but no single treatment results in predictable and satisfactory outcomes, especially for problematic keloids. A high therapeutic response rate without major complications was identified in this study, suggesting that cocktail therapy with bleomycin and verapamil can be considered as a safe and effective treatment modality for keloid scars. Moreover, this method has considerable potential for being combined with other regimens, such as surgical excision or radiotherapy, to produce superior outcomes.

Characteristics of keloid patients treated with triamcinolone
Notes
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was performed in accordance with the principles of the Declaration of Helsinki.
Patient consent
The patients provided written informed consent for the publication and the use of their images.