INTRODUCTION
Nasal deviation is a condition where the axis of the nose deviates from the midline. It can be difficult to correct with rhinoplasty. Nasal deviation is caused by a defect in either the upper (bony) or lower (cartilaginous) part of the nasal framework, or both (osteocartilaginous) [1]. Surgical management is determined by the part involved. Correction and maintenance of the bony portion require osteotomy and a rigid support structure. To accomplish this, many osteotomy and bone grafting methods have been introduced. The authors investigated a method that yielded satisfactory results. In this method, the septum is supported by moving a wedge-shaped nasal bone that is created by osteotomy and uses it as a graft to supplement the bony defect on the opposite side; this places the bony framework and the septum at the midline in patients with a bony deformity and septal deviation.
METHODS
Among patients who underwent corrective rhinoplasty from October 2014 to June 2015, ten were selected for medial and paramedian osteotomy because their septums and bony junctions had deviated from the midline, although the computed tomography (CT) results indicated that lateral osteotomy was unnecessary because both the lateral walls were relatively symmetric (Fig. 1). All the patients were males, and the average age was 31.9 years. We confirmed the correction of a deviation with pre- and postoperative photographs, and scored patient satisfaction and colleagues’ evaluations of the surgical results using a 5-point Likert scale.
Surgical procedure
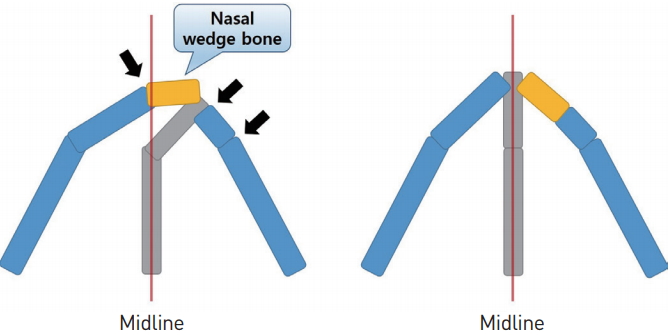
Under general anesthesia, patients underwent wide exposure up to the bony framework using an open rhinoplasty technique. After infiltration of 2% lidocaine mixed with 1:100,000 epinephrine, a transcolumellar incision and two marginal incisions were made. Septal dissection was performed to separate both the medial crura, and subsequently the bony portion was exposed. The mucoperiosteal flap was sufficiently undermined to prevent nasal synechia. After separating the upper lateral cartilage and septum, we performed a medial osteotomy and bilateral paramedian osteotomy via a reciprocating saw and an osteotome on the bony deviation that was confirmed on preoperative CT. Thus, a wedge-shaped bone was separated at the side where the medial and paramedian osteotomies were performed. The average width of the bone graft was 3 mm. We placed the nasal septum in the midline using the swinging door maneuver and supported the bony framework by inserting the excised wedge-shaped bone graft in the bony defect area (Fig. 2). When the patient requested correction of the nasal tip, we also performed a tip plasty with a columellar strut, tip onlay graft, or shield graft. The patients were all discharged three days after surgery.
RESULTS
Surgery was performed with this method on 10 patients, and the average follow-up period after surgery was 5.4 months (1 to 10 months). Photographs were taken, and physical examinations were performed before surgery, and 1, 3, and 6 months after surgery. Patient satisfaction and colleagues’ evaluations of the surgical results were measured using a 5-point Likert scale (very satisfied, satisfied, neutral, dissatisfied, or very dissatisfied).
The average score of the patients was 4.6, and all the patients were either very satisfied or satisfied (Table 1). Most of the nasal deviations showed improvement and an overall reduction in size or dorsal depression did not occur on photographic review (Fig. 3-5). The mean score of our colleagues’ ratings was 4.2 points. After surgery, some patients complained of hypesthesia, but there were no significant complications.
DISCUSSION
Nasal deviation is deviation of the nasal pyramid from the facial midline [2]. Osteotomy (medial, lateral, intermediate, double, percutaneous, and/or continuous) plays an important role in correcting an irregular bony framework [3]. Nevertheless, deviation may recur after surgery because of the “memory” retained by the nasal pyramid relative to the surrounding original soft nasal tissue, and this problem may be the most difficult part of corrective rhinoplasty. In other words, the soft tissue attachment (e.g., the nasal skin, mucous membrane, and periosteum) has a tendency to revert to the original deviation. This can be induced by postoperative contracture and other factors [2]. To reduce the recurrence of deviation, surgeons have developed new techniques, such as septocolumellar suturing [4] and have performed more delicate bone work using microperforating osteotomy techniques [5]. A new osteotomy method including beveled bone resection has also been introduced [6].
In rhinoplasty, bone grafting was first performed in 1975 by Sheen [7]; this procedure reconstructed the nasal tip using bone from the nasal radix. Since then, various methods including transplantation of a rib graft into the alar collapse region [8], septum reconstruction with a radial bone [9], and spreader grafting with an ethmoid perpendicular plate [10] have been introduced and are widely performed.
Our method, other than using autologous tissue, does not require another donor site to achieve a rigid bone graft and has the benefit of using resected bone for correction. Very small bone grafts are reportedly resorbed, but this mainly seems to have occurred when the graft was transplanted into the tip region [11]; we performed transplantation at the dorsum, which moves less than the tip and has good blood flow, reducing the likelihood of resorption. Although the authors were trying to record a follow-up CT to prove this, every patient rejected taking a CT as a matter of cost and radiation. It was confirmed that the location of the graft was maintained in a physical examination and photographic review after surgery.
Because this method does not include lateral osteotomy, both the lateral walls solidly support the bony framework; however, because the method corrects midline deviation at the bony septal junction by only using paramedian osteotomy, it is important to pre-select a candidate who meets the criteria for surgery. A thorough preoperative physical examination, photography, and CT enabled us to select patients who had severe midline deviations as candidates for surgery, even though both lateral walls were relatively symmetric.
We performed taping and splinting after surgery to prevent migration and malpositioning of the graft. We are considering suture fixation using a drill to solidly attach the graft. Although the small number of cases is a limitation, this method show promise as an effective technique in the correction of nasal deviation because it is simple, effective, and long-lasting, when properly performed.
CONCLUSION
In corrective rhinoplasty, proper osteotomy and repositioning of the bony portion are very important. However, medial and lateral osteotomy are not required in all cases; depending on the patient’s condition, by performing only medial and paramedian osteotomy and transplanting a wedge-shaped nasal bone graft onto the opposite side, we effectively corrected and supported the bony framework and confirmed maintenance of the position.
This method proved successful in providing satisfactory results; we expect to improve the technique by performing more cases in the future.