INTRODUCTION
The abdomen is the one of the most common areas treated in plastic surgery procedures. In recent years, abdominoplasty has been increasingly used to manage abdominal hypertrophy, laxity, and striae [1,2].
After pregnancy or weight changes, patients often desire improvement of abdominal striae and laxity, including the repair of additional ventral hernias.
It is reasonable for postpartum middle-aged women to request some extent of lower abdominal tightening without major surgery, along with the removal of multiple striae on the mid lower abdomen and periumbilical area. Many modalities have been used to correct unsightly striae of the lower abdomen, including laser treatments, intense pulsed light, micro-dermabrasion, and some homemade cream regimens. However, the results of those methods are generally unpredictable [3].
For patients who would like to achieve favorable cosmetic outcomes of unsightly visible multiple postpartum striae on the lower mid-abdomen, and to improve their protruding belly contour by tightening of the lower abdomen, we designed the keyhole-shaped vertical mini-abdominoplasty, and herein we report our initial clinical experience.
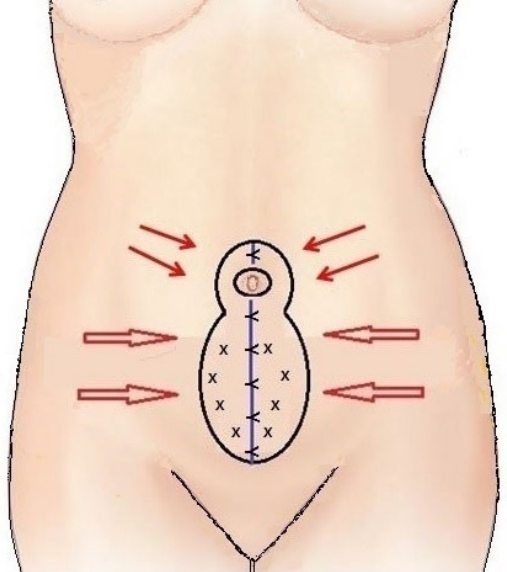
This novel abdominoplasty technique was performed in a patient with multiple postpartum striae on the lower mid-abdomen and periumbilical area. The keyhole-shaped vertical mini-abdominoplasty was designed as follows. First, the striated skin expected to be excised was measured by carefully pinching the lower abdominal skin with the patient in the upright and supine positions. Using a surgical marker, a keyhole-shaped abdominal marking for skin incision was made, including the internal periumbilical circumferential incision. A tumescent solution of 1:100,000 epinephrine diluted with saline was infiltrated into the surgical field (Fig. 1).
CASE REPORT
A 37-year-old woman presented with typical multiple striae on the lower mid-abdomen and periumbilical area, as well as mild bulging in this area. She had given birth to two children and had a preexisting Pfannenstiel incision scar in the lower abdomen, a history of operation for umbilical hernia 7 years ago, and a relatively long distance between the symphysis and the umbilicus. Her body mass index (BMI) was 20.6 kg/m2.
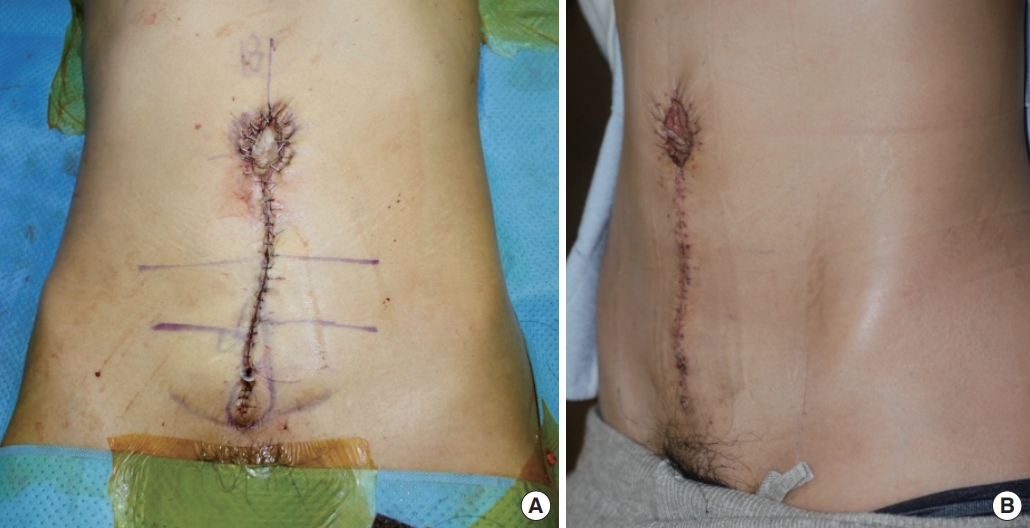
The keyhole-shaped abdominoplasty including the area of multiple striae on the mid-abdomen and umbilicus was designed. The incision was made starting from the lower pole of the keyhole design, and an area of multi-striated lower abdominal and periumbilical skin, measuring approximately 10×15 cm2 and weighing about 450 g, was excised. Midline reinforcement of the loosened anterior rectus sheath with 3-0 Prolene sutures and plication sutures on the abdominal wall was done. Both lateral abdominal skin flaps were medially advanced to close the skin defects. During direct suture approximation of both lateral skin flaps, a small dog-ear deformity (3×1 cm2) on the inferior portion of the skin suture line was removed by elliptical excision (Figs. 2, 3). Postoperatively, the patient had a favorable lower abdominal appearance with a marked reduction of striae on the abdominal and periumbilical area and an aesthetically favorable, flat lower abdomen. At 4.5 months after the operation, relatively good results were maintained (Figs. 4, 5).
DISCUSSION
Striae gravidarum, also known as stretch marks, occur in 50% to 90% of postpartum women [4,5] despite the numerous preventive methods during pregnancy that have been developed. These striae are caused by skin stretching and the effects of hormonal changes on skin fibers during pregnancy. Stretch marks on the abdomen may cause patients to have a distorted body image and are a source of significant anxiety for women, with significant impacts on their quality of life. They are caused by tearing of the dermis, and begin as reddish-purple lesions, after which they eventually develop into streaks of pale atrophic scars.
Although many methods have been used to treat striae, such as laser treatment [6,7], intense pulsed light, micro-dermabrasion [8], and some topical cream regimens [9], there is still no established technique for preventing or treating this problem.
Abdominoplasty is frequently performed to improve the abdominal wall contour, to construct a natural-appearing umbilicus, and to restore other anatomical deformations of the abdomen. Numerous variations and modifications of abdominoplasty procedures have been developed. To achieve the optimal postoperative results, careful selection of the appropriate technique for each individual case is required [10-12].
This study reports the case of a woman who had moderate to severe striae gravidarum in the lower abdomen and peri-umbilical area with mild laxity, no tissue excess of the lower abdomen, and some degree of a bulging belly. She had given birth to two children and her BMI was 20.6 kg/m2, within the normal limits. The patient received an explanation regarding the resulting midline straight abdominal scar, including the possible occurrence of hypertrophic scars, and she chose to undergo the procedure.
Preoperatively, the width of the expected skin resection including the area with many striae with appropriate tension that will not interfere with normal wound healing was evaluated by careful pinching of the abdomen tissue by the patient herself and the surgeon. Then, the keyhole-shaped incision marking was made with the patient in the upright position. Intraoperatively, the patient must flex at the level of the hips to loosen the tension of the abdomen. After the resection of horizontal skin excess in a vertical direction, the loosened anterior rectus sheath was identified. The loosened anterior rectus sheath was reinforced with running reinforcement 3-0 Prolene sutures, and multiple plication sutures were made on the anterior abdominal wall. During approximation of the skin sutures, the potential occurrence of a dog-ear deformity at the inferior distal suture line should be considered. The medial advancement of both lateral skin flaps for skin closure tightened and improved the waistline. At postoperative 4.5 months, marked reduction of the lower abdominal and umbilical striae was observed, as well as a flatter abdomen than before the operation.
This keyhole-shaped vertical mini-abdominoplasty is characterized by a vertical incision along the midline of the lower abdomen. Originally, the results of this technique were limited to the reduction of moderate to severe striae on the mid-abdomen. During in this techniques, lipoplasty can be simultaneously performed with or without liposuction. Optimal candidates for the keyhole vertical mini-abdominoplasty are postpartum women in their late 30s to middle age who have a normal BMI, moderate striae on the lower mid-abdomen and periumbilical area, and mild to moderate bulging and skin excess on the mid-abdomen.
The principal contraindications of this operation are a disposition to keloid or hypertrophic scarring, and the patient’s unwillingness to accept a vertical midline postoperative scar.
This method is a definitive technique for the removal of striae, and yields longer-lasting improvements for lower abdominal striae than other modalities. Furthermore, it also results in an aesthetically appealing, flat lower abdomen and an improved waistline.
Before the operation, the physician should inform the patient about the possible occurrence of keloids or hypertrophic scars, and patient must accept the vertical mid-abdominal postoperative scar associated with this procedure. It is also important to assure the patient that the final resulting midline abdominal scar will have a better appearance than multiple striae in the mid-abdomen. The need for periodic careful follow-up visits for scar management should also be emphasized.