INTRODUCTION
Breasts are important for women in terms of both functional and aesthetic aspects, the latter of which can also have psychological implications. The nipple is one of the most important factors affecting the function and shape of the breast. Some women experience emotional distress associated with their nipple size or shape, especially if it is large or ptotic. The epidemiology of nipple deformity is unknown, but it seems to be common in Asian populations [1]. In women who experience psychological stress due to the shape of their nipples, nipple reduction surgery could be very helpful.
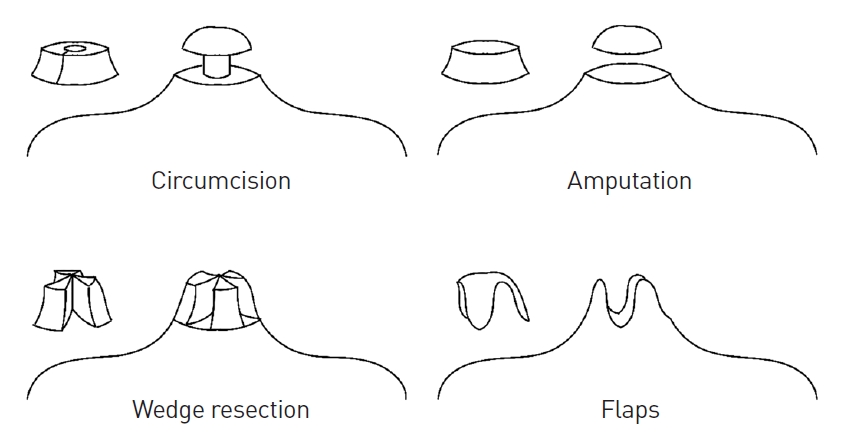
There are four major surgical techniques for nipple reduction: circumcision, amputation, wedge resection, and flaps [2]. These four techniques are illustrated in Fig. 1. Each technique has advantages and disadvantages, which are mainly associated with the aesthetic outcome, preservation of lactiferous ducts, and complexity of the surgical technique. Although aesthetically unsatisfactory results and scarring/contracture have not been described for any surgical techniques, it is reasonable to presume that wedge resection and flap techniques may result in postoperative surgical scars due to their asymmetric design [3-5]. Regarding the patency of lactiferous ducts, which is especially important in breastfeeding women, circumcision, amputation, and wedge resection may impair the ability to lactate. Although the flap and wedge resection techniques involve complicated surgical techniques, we regard this aspect as a relatively unimportant issue when considering their more satisfactory outcomes. From the perspective of these considerations, we present a novel technique that has benefits in terms of its symmetric design, resulting in good aesthetic outcomes, and preservation of the lactiferous ducts, enabling breastfeeding.
IDEA
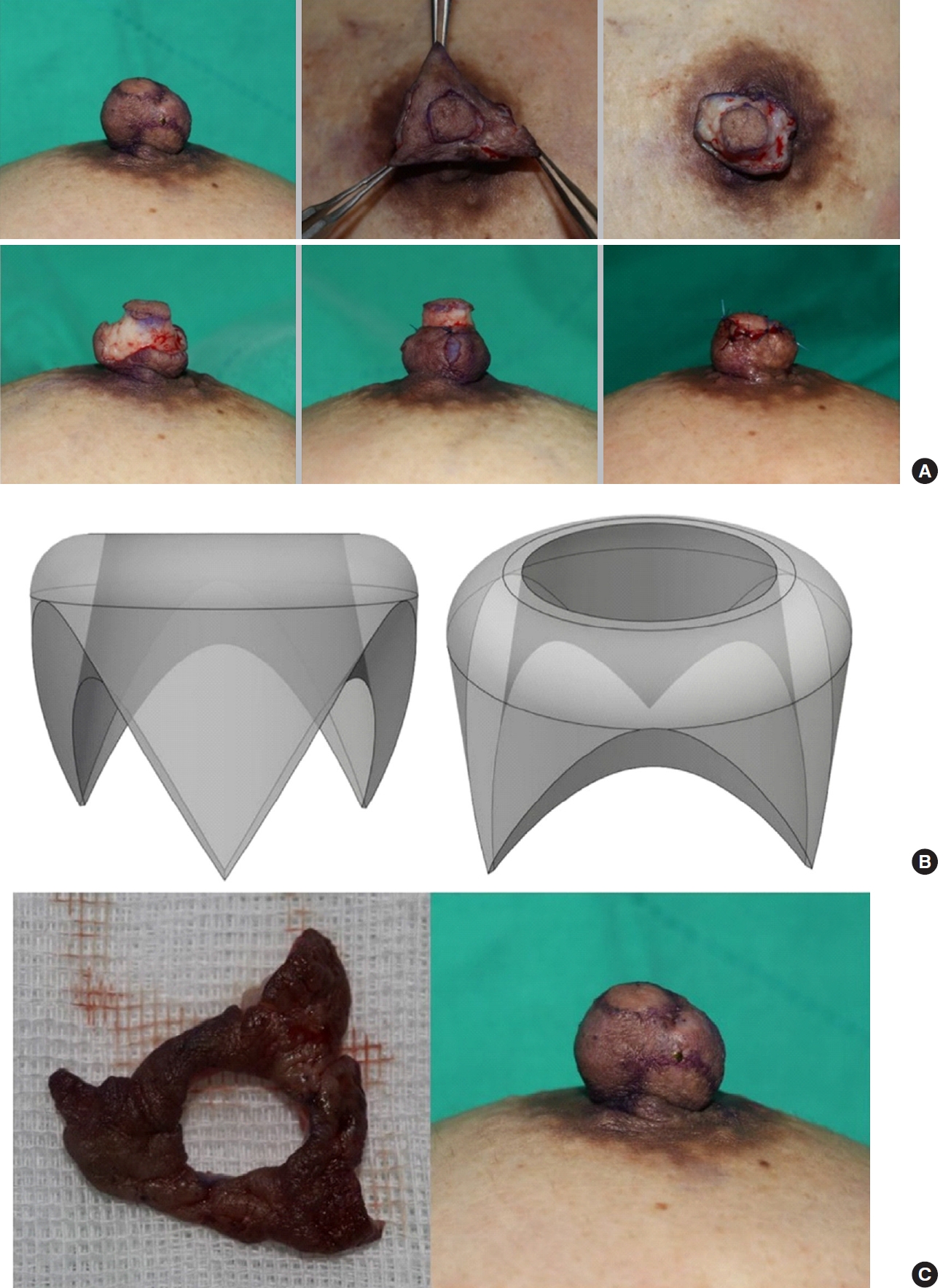
A 43-year-old woman presented with large nipples (macrothelia). This patient had experienced psychological distress associated with the size and ptosis of her nipples. Clinical photographs were taken preoperatively (Fig. 2A), intraoperatively (Fig. 3A), and at 1 month after the operation (Fig. 2B). Before surgery, we had a consultation with the patient about the expected postoperative result. The surgical design was done intraoperatively and complete stitch removal was performed at 2 weeks postoperatively.
Surgical technique
The incisional design for the tripod wedge resection is composed of three triangular legs (tripod) and one doughnut-shaped head (Fig. 3B and C). By varying these factors, the operator could manipulate the length and width of the nipple. With our design, the skin was resected primarily and then the soft tissue was excised, followed by an additional excision of soft tissue that made volume management possible.
After excision of soft tissue with an appropriate volume of the nipple, the remaining lateral skin of the nipple was repaired with each other so that the nipple looks like a telescope. Before repairing the skin flaps on the top and lateral walls, the operator could imagine the final shape of the nipple. Because of the tension between the skin flaps on top and the lateral wall, the length of the nipple was shortened, and the width of the nipple was increased compared with the remaining soft tissue that was trimmed. An antibiotic ointment was applied on the reduced nipple and a foam dressing with a nipple-sized hole was applied for nipple protection.
Assessment
This technique was carried out for the first time in this case. The patient experienced alleviation of emotional distress and was satisfied with the surgical outcome. From an aesthetic standpoint, the length, diameter, and severity of ptosis all improved. There were no surgical complications associated with aesthetic factors, such as asymmetry or inversion of the nipple induced by scarring or contracture. The circumference and length of the nipple were reduced postoperatively, resulting in a clear improvement in the degree of ptosis.
Regarding the functional aspect of the nipple, there are two things to consider. First, with regard to the patency of the lactiferous duct, it was not possible to confirm directly whether breastfeeding was possible in our case, but our surgical technique does not involve the lactiferous duct. Therefore, it is almost certain that breastfeeding would be possible after this procedure. Second, with regard to sensory changes of the nipple, the patient experienced numbness of the nipple for about 2 weeks, but after approximately 1 month, the sensation of the nipple recovered to its normal preoperative status.
DISCUSSION
Although nipple reduction is necessary for women who experience distress due to protruding nipples, techniques for nipple reduction vary since there is no standard method considering both symmetric cosmetic results and functional aspects such as preservation of the lactiferous ducts (Table 1). This novel technique is favorable from both standpoints. Regarding the cosmetic aspect, our method was able to decrease both the length and diameter of the nipples, and we used an evenly tensioned incision line to obtain a symmetric aesthetic outcome.
Although the amputation technique, as exemplified by the chullo-hat method, can maintain symmetricity, it can only decrease the length of nipples and also poses a risk of sensory loss that is not present in our method [6,7]. Conventional methods such as the sinusoidal flap incision technique [4,8] may have complications related to postoperative asymmetric contracture. From a functional standpoint, some techniques, including circumcision and some types of vertical wedge resection [9,10], may avoid lactiferous duct injury, as is also the case for our method. However, the circumcision method cannot decrease width; instead, it only reduces length. Likewise, the vertical wedge resection method can only reduce width, but not length. In our method, the width of the circular doughnut-shaped skin tissue, which lies on top of the three legs, is the factor responsible for decreasing nipple width, while the length of the three legs is the factor responsible for decreasing nipple height. Therefore, considering both the aesthetic aspect and the functional aspect, especially for patients who plan to breastfeed in the future, our tripod wedge resection technique can be a good surgical method.
There are some limitations to this study. First, a measurement or grading of the patientŌĆÖs preoperative status was not available. Considering the novelty of this method, accurate measurements of the preoperative and postoperative status may be needed in further evaluations. When more cases are analyzed in the future, it may be possible to evaluate the degree of satisfaction in terms of grades and their distribution. This method may also seem complicated to less skilled surgeons, and standardization of this novel method may be needed to achieve consistent results.
The tripod wedge resection method, a novel technique for nipple reduction surgery, could become the standard method once its technique is standardized, since it has numerous advantages including symmetric results, decreases in length and diameter, and the avoidance of injuries to the lactiferous duct. Further efforts to apply this method more widely and to analyze the results accordingly may contribute to the establishment of an efficient and safe nipple reduction technique.