INTRODUCTION
Keloid is a scar tissue that undergoes recovery and excessive growth over the original wounds when the collagen is excessively accumulated in the dermis during the wound healing process. Unlike hypertrophic scar that is limited to the sites of injury and achieves a recovery over time, keloid is characterized by no changes in the size over time [1]. It may occur with no respect to the age and shows a predilection in individuals aged between 10 and 30 years. The causative factors include skin injuries due to surgery, laceration, tattooing, injections and prophylactic vaccination, excessive skin tension and hormonal imbalance [2]. It commonly affects individuals with genetic predisposition. The common sites of occurrence include the anterior thorax, shoulder, upper extremities and ear [3] To our knowledge, however, there are few cases of keloid that occurs in the axilla. In addition, there are fewer cases of keloid that bilaterally occurs at the operated sites postoperatively in individuals with no past or family history. But, we experience with a rare case of keloid occurring in the axilla after osmidrosis surgery and then we report our case with a review of literatures.
CASE
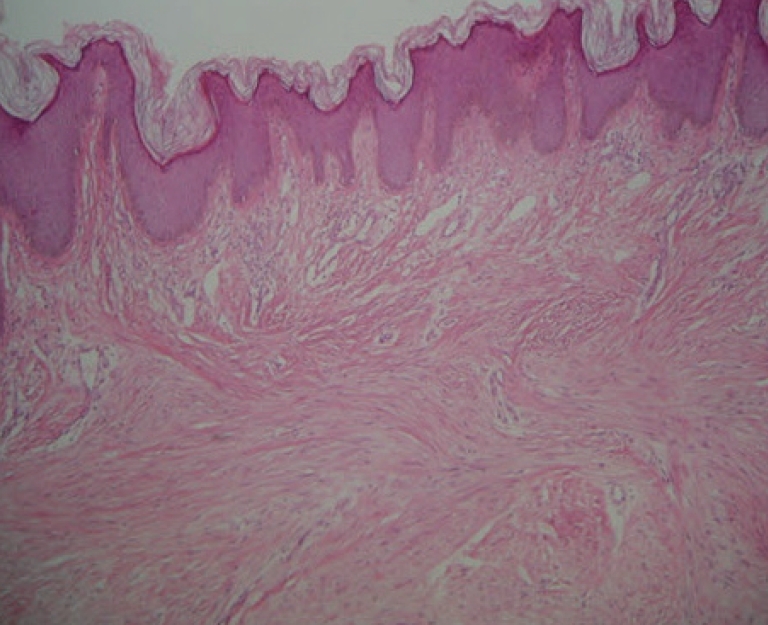
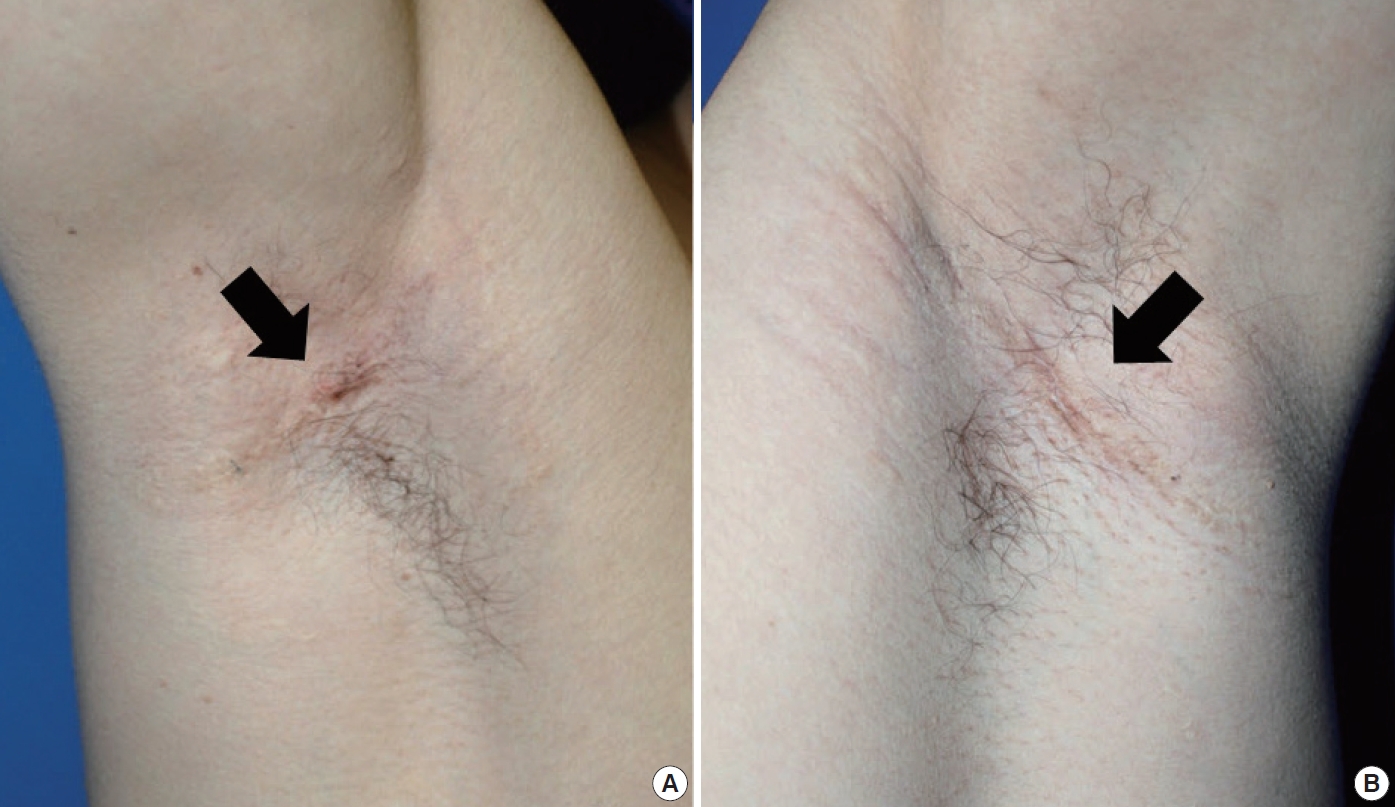
A 21-year-old man visited us with a chief complaint of a keloidlike scar formed in the bilateral axillae. On history taking, the patient underwent subdermal shaving two years ago for the management of osmidrosis but had not received appropriate scar management during the military service. The mass had occurred six months before outpatient visit and then it had slowly grown, for which the patient had not received any appropriate treatments. At the time of outpatient visit, the patient complained of pruritis at the sites of scar formation. But the patient presented with no other specific symptoms. On family or past history, the patient had no notable findings associated with keloid. Moreover, the patient also had no notable findings at a preoperative work-up. On physical examination, the patient had a tenderness and he also had a glossy, pinkcolored, firm, oval-shaped, well-defined mass of 5.0├Ś1.5├Ś0.5 cm in size in the right axilla and 5.0├Ś2.0├Ś1.0 cm in size in the left axilla (Fig. 1). Based on the physical examination and the morphology of the mass, we assumed that it would be highly probable that the mass might be a keloid-like scar that occurred postoperatively. We therefore planned combination treatments of surgery with steroid injections. Under intravenous anesthesia, we performed intralesional excision. This procedure leaves the outer segment of the keloid, cutting out the central portion of the scar. At the time of surgical excision, the wound bed and margins in the bilateral regions, were injected with a small amount of intradermal triamcinolone acetonide 40 mg/mL diluted to 10 mg/mL. To compress the operated sites, the gauze was applied in a fluffy ball shape on both sides of the axilla and followed by dressing using an elastic bandage. On gross finding, cross sections of the mass contain homogeneous fibrous materials. In histopathological report, no flattening of the overlying epidermis, and presence of keloid collagen which confirms diagnosis of keloid (Fig. 2). During the regular follow-up period, the patient was given steroid injections twice more at a 3-week interval. Three years postoperatively, the patient currently presented with no recurrence or other notable episodes (Fig. 3).
DISCUSSION
Keloid was first described in the days of the ancient Egyptian empire. In addition, it was first coined, by Alibert in 1806, to describe its overgrowth into the adjacent normal tissue (from the Greek chele, meaning ŌĆ£crabŌĆÖs clawŌĆØ) [4]. Currently, it is referred to as fibrous hyperplasia after the onset of skin trauma due to various etiologic factors. The causative factors include skin injuries due to surgery, laceration, tattooing, injections and prophylactic vaccination, excessive skin tension and hormonal imbalance. Still, however, little is known about the exact mechanisms by which the keloid is formed [2]. It has been hypothesized that it occurs as a result of the derangement in the growth factor control, abnormal collagen synthesis, abnormal immune response and the abnormal functions of the sebaceous gland.
Once developed, keloid shows a high rate of recurrence and causes many cosmetic problems because no complete cure can be achieved. It is therefore important to make a differential diagnosis between keloid and hypertrophic scar. Keloid can be differentially diagnosed from hypertrophic scar based on the clinical and histopathologic characteristics. Hypertrophic scar is characterized by its location limited to the initial wounds and occurs within the first four weeks after the onset of the injury. But keloid shows excessive growth over the initial wounds and is formed after four weeks from the onset of the injury. Moreover, hypertrophic scar is decreased in size within one year. But keloid is not decreased in size for more than one year [1]. Histopathologic examinations show that both keloid and hypertrophic scar are characterized by the increased fibrous bundles. However, keloid is characterized no flattening of the overlying epidermis, no scarring of the papillary dermis, keloid-like collagen fibers, fibrous bands like fascia and the irregular arrangement of fibrous bundle. In the current case, the mass had the histopathologic findings that are suggestive of keloid; these include abundant collagen fibers and the irregular arrangement of fibrous bundle. But it occurred in the axilla rather than the anterior chest, shoulder, upper extremities and ear, all of which are considered the common sites of occurrence of keloid. To our knowledge, our case is rare in that it occurred bilateral axillae to the operated sites despite a lack of both a past and a family history. Then, we assume that the causes of keloid as shown below:
1) The patient could not receive the treatments for wounds after undergoing surgery for osmidrosis during the military service. It is therefore highly probable that the inflammations might have occurred at the operated sites.
2) The patient did not receive the appropriate treatments for the inflammatory responses. But we experience limitations in identifying the causes of keloid in the current case.
As the treatment modalities for keloid, surgery has been used the most commonly in patients with keloid. It has been reported, however, that surgery alone causes a higher rate of recurrence of 45-100% [5]. Therefore, local steroid injections are frequently used as adjuvant therapy to surgery for the purposes of inhibiting the expression of collagen genes in patients with keloid [6]. Chowdri et al. reported that the recurrence rate was 8.1% during a follow-up period of 30 months following a concomitant use of surgery with local steroid injections, thus advocating the efficacy of the combination of the two methods [7]. It can therefore be stated that the combination of surgical excision and local steroid injections is currently the most popular modality. Although the keloid was effectively removed, it is characterized by long-term recurrence. Therefore, the follow-up period would be a key factor. It has been reported that 5.5-12.9 months elapsed on average until the recurrence following the treatment [7]. At our institution, there were no notable episodes such as tissue atrophy, telangiectasia formation, hypopigmentation, and recurrence during a 3-year follow-up period.
As shown in our case, there is a possibility that keloid might occur in the axilla. Therefore, keloid formation after axillary operation deserves special attention. In the current case, keloid was formed after approximately one year and six months postoperatively. It can therefore be inferred that both short-term treatments of the operated sites and a long-term regular follow-up would be essential. In addition, although unclear, insufficient or inappropriate postoperative management would lead to the formation of keloid scar. Then, postoperative care also deserves special attention.
We experienced a rare case of keloid occurring in the axilla and then successfully treated it with intralesional excision and local steroid injections. Here, we report our case with a review of literatures.