INTRODUCTION
Trap-door deformity is a biophysical phenomenon in which U-, C-, or V-shaped linear scars tend to become depressed and the tissue circumscribed by them tends to bulge. The trap-door effect takes its name from its similarity to the effect of lifting or sliding a door that covers an opening in a roof or floor [1]. This effect seems to be caused by the concentric retraction of a curved scar, which gives rise to an outward bulge that projects above the surrounding skin surface. Non-surgical first-line treatments are considered before performing various surgical corrections for patients with trap-door deformity. The injection of triamcinolone acetonide (TCA), which has been established to facilitate collagen degeneration, and subcision can be considered as a treatment option since circular contracture plays a significant role in the mechanisms underlying trap-door deformity [2,3]. However, insufficient research supports this treatment modality. Therefore, the aim of the present study was to demonstrate the efficacy of TCA injection and subcision as a first-line treatment for post-traumatic acute trap-door deformity.
METHODS
Patients
From December 2013 to October of 2015, 12 patients visited our scar clinic with trap-door deformity. A single plastic surgeon diagnosed trap-door deformity (i.e., a significant bulging accompanied by a semicircular, U-shaped, or V-shaped scar), and the treatment was then started.
Treatment
First, a subcision was performed; this procedure involves cutting the fibrotic band along the scar line in the depression using a 22-gauge needle (Fig. 1A). The authors made the subcision in 2 directions (Fig. 2): vertically and tangentially along the depressed scar line. After the subcision, patients immediately received a TCA injection using a 30-gauge needle (0.1ŌĆō0.3 mL, Tamceton┬« [Hanall Pharmaceutical, Seoul, Korea]) diluted with 2% lidocaine to a concentration of 20 mg/mL in an effort to reduce pain (Fig. 1B). An intralesional injection was administered in areas of scar tissue that were difficult to penetrate with a needle. The depth of the injection was strictly limited to the scar area to avoid atrophy of the normal subcutaneous tissue. The interval between the injections was 2 weeks or longer, and the number of injections depended on the degree of improvement of the trap-door deformity; however, a maximum of 6 injections were administered. The treatment was terminated when the plastic surgeon determined that no further treatment was needed, or when the patient was satisfied with the scar or refused further treatment.
Treatment evaluation (scar evaluation)
The primary scar quality parameters were obtained at each follow-up visit by the same plastic surgeon who performed the procedure using the subjective patient and observer scar assessment scale (POSAS) [4]. Because bulging was one of the main parameters that we expected to correct, we used an additional question to evaluate bulging, in addition to the patientŌĆÖs and observerŌĆÖs general opinion. Bulging was evaluated by assigning a score to the most protruding part of the trap-door deformity area in comparison with the same area on the opposite side. In the general opinion item, a score was used to evaluate the overall improvement of the scar and the approximate level of satisfaction before and after treatment. The POSAS consists of 2 numeric scales: the patient scar assessment scale (patient scale) and the observer scar assessment scale (observer scale). The patient and observer scales must be completed by the patient and observer, respectively. Each item has a 10-point score, whereby a score of 10 represents the worst imaginable scar or sensation. The total score of the observer scale is obtained by adding the scores of each of the 5 items (score range, 5ŌĆō50). The total score of the patient scale is obtained by adding the scores of each of the 6 items (score range, 6ŌĆō60). The lowest scores, 5 and 6, respectively, represent normal skin. In order to make the assessment more specific to trap-door deformity, the observer and patients reported a score regarding bulging as well as their general opinion on the appearance of the scar areas (score, 1ŌĆō10; with a score of 10 corresponding to the worst possible scar appearance).
RESULTS
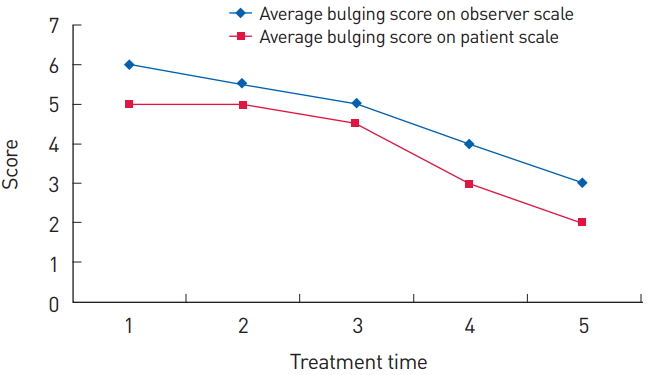
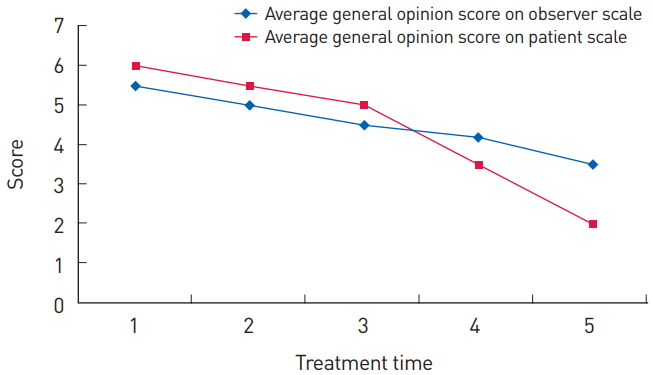
The patientsŌĆÖ mean age was 41.5┬▒20.56 years (range, 15-72 years); 8 were men and 4 were women. The average time to treatment after the traumatic injury was 2.67┬▒0.78 weeks, the average treatment period was 8.75┬▒1.48 weeks, the average follow-up period after the last treatment was 7.25┬▒3.36 months; and the average number of treatments was 4.08┬▒0.51 (Table 1). The average POSAS score per question on the observer scale improved from 6.6┬▒1.31 to 3.6┬▒1.08, and the average POSAS score per question on the patient scale improved from 5.5┬▒1.57 to 2.5┬▒1.26 (Fig. 3). The average bulging score on the observer scale decreased from 6.0┬▒0.98 to 3.0┬▒0.83, and that on the patient scale decreased from 5.0┬▒1.67 to 2.0┬▒1.30 (Fig. 4). The average general opinion score on the observer scale decreased from 5.5┬▒1.12 to 3.5┬▒0.91, and that on the patient scale decreased from 6.0┬▒1.84 to 2.0┬▒0.79 (Fig. 5). Additional surgical correction was not required in any patient, and treatment was terminated in all patients. There was no recurrence of bulging or other symptoms in the follow-up period.
Case 1
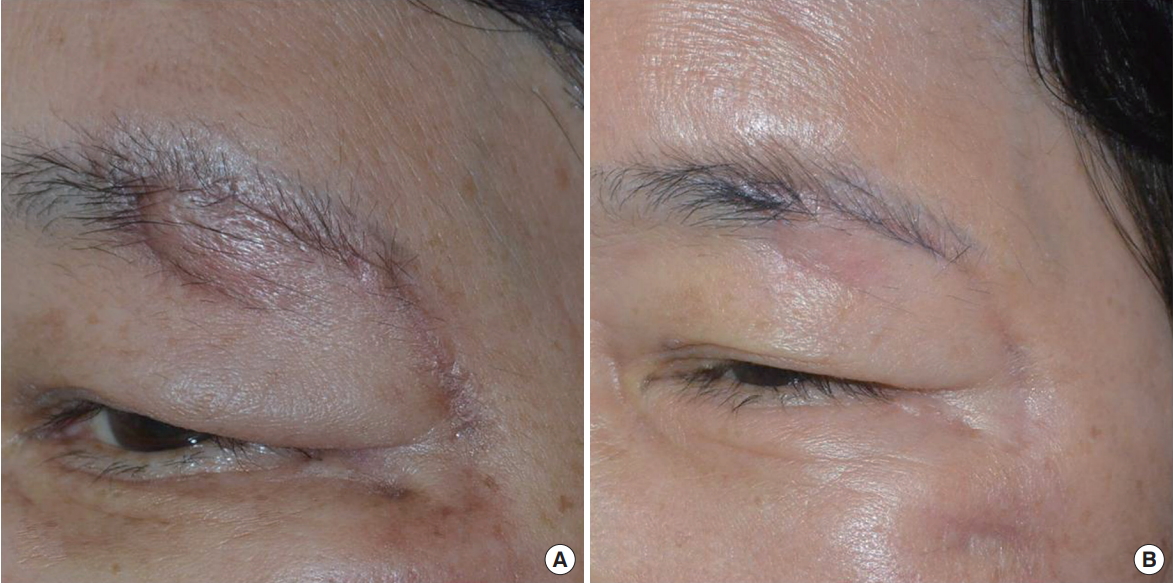
A 63-year-old woman suffered a left blowout fracture with a laceration on the left eyebrow (Fig. 6). The laceration was sutured on the day of the trauma in the emergency room. Two weeks after the trauma, treatment was started. In 8 weeks, 4 rounds of treatment were done. The treatment was terminated because the plastic surgeon determined that no further treatment was needed.
Case 2
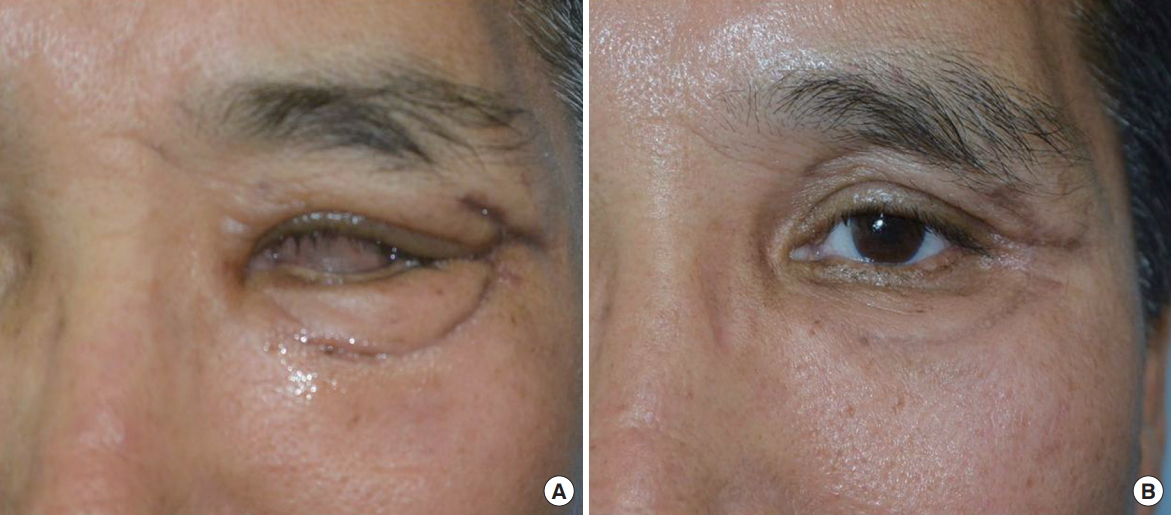
A 59-year-old man had a severely comminuted left orbitozygomatic fracture with multiple lacerations on the left periocular area (Fig. 7). The laceration was sutured on the day of the trauma in the emergency room. Three weeks after the trauma, treatment was started. In 12 weeks, 5 rounds of treatment were done. The treatment was terminated because the plastic surgeon determined that no further treatment was needed.
DISCUSSION
It is important to know the etiology of trap-door deformity to perform adequate treatment. Various explanations have been proposed for trap-door deformity. Early studies focused on factors such as lymphatic and venous obstruction, excessive subcutaneous fat, a beveled wound edge, and hypertrophic scarring [1,2,5]. However, trap-door deformity can develop regardless of whether the semicircular incision has an inferior or superior base, and it may occur several months after the wound has healed, with no relationship to tissue elevation inside the scar that seems edematous due to lymphatic and venous obstruction [6]. Moreover, these proposed causative factors were disproved by subsequent studies showing that trap-door deformity recurred after defatting or revision of scar hypertrophy [7,8].
Recent studies have focused on trap-door deformity due to scar contracture. Koranda and Webster [2] suggested that there are usually 3 planes of contracture in a scar: vertical, longitudinal, and horizontal. The contractile forces of the longitudinal and horizontal planes seem significant. Webster et al. [5] demonstrated that 3 factors (the unique retraction of curved scars, the interruption of tension lines by a curved scar, and the effect of local movement) play an important role in the formation of trap-door deformity, and they emphasized the importance of the complete removal of contracted tissue for surgical correction. Numerous studies have been conducted on the effects of surgical correction on trap-door deformity. Aus├Łn [1] used multiple Z-plasty or saw-toothed incision instead of the traditional W-plasty after multiple serial excisions, and she proposed that W-plasty plays an important factor in the etiology of trap-door deformity by reducing contracture. Lee et al. [9] proposed using W-plasty and Z-plasty after surgical debulking once the flap has been re-evaluated. Webster et al. [5] described a preventative technique for trap-door deformity using 2 Z-plasty incisions. These surgical corrections are definitive solutions, but if the length of the scar becomes extended or if the U-shaped or V-shaped scars cannot be improved, trap-door deformity has a high likelihood of recurring. In addition, when patients are eager to treat the scar, waiting 3 to 6 months for scar maturation could be burdensome for both surgeons and patients.
Nevertheless, Koranda and Webster [2] and Webster et al. [5] also agreed that the complete removal of scar contracture is crucial for treating trap-door deformity; thus, a TCA injection and subcision could be very important during this procedure, and most patients showed good results without undergoing surgical correction.
Corticosteroids inhibit ╬▒2-macroglobulin, which in turn inhibits collagenase. Once this pathway is blocked, collagenase become activated, thus facilitating collagen degeneration [10]. The efficacy of corticosteroid injections in the treatment of scars has been well established, and the most commonly used corticosteroid is TCA [3]. We mixed TCA with lidocaine and used this mixture, because injecting TCA with lidocaine greatly reduces the pain of the injection, enabling patients to tolerate multiple needle pricks. The local complications of TCA injections include atrophy of the adjacent skin, depigmentation, pigmentation, and telangiectasia, whereas systemic complications include weight gain, diabetes, and Cushing syndrome. In our study, we observed no TCA-related complications, perhaps because of the long injection interval and the small dose of TCA that was used.
Subcision is a safe, easy-to-perform, well-tolerated, and effective surgical technique for select depressed scars. Defined and described by Orentreich and Orentreich [11], subcision is a method for subdermal undermining of depressed areas. The process, as modified by us, entails introducing a tri-beveled hypodermic needle just under the dermis to release fibrous attachments tethering the epidermis and dermis to the subcutis. The back-and-forth motion of the needle parallel to the skin results in audible rasping and popping as the underside of the dermis is released from its attachment to the subcutis [12]. Subcision corrects a depressed scar through 2 mechanisms. The first mechanism is the surgical act of cutting under and releasing the tethered site, and the second mechanism is new connective tissue formation [11]. We performed subcision in 2 directions: vertically and tangentially along the depressed scar line to maximize the cutting effect. The disadvantages of subcision are bruising and, occasionally, a hypertrophic reaction. Therefore, we minimized bleeding by using a mild compression and an ice pack after subcision, and we administered a TCA injection to prevent hypertrophic scarring.
Thus, using TCA and subcision together as an early treatment can eliminate some issues with the current surgical correction methods. However, this study has an important limitation. The POSAS was used to assess the therapeutic effect, but it is a more appropriate evaluation for burn scars or linear scars [4]. Patients are most uncomfortable with bulging, and surgeons focus on treating bulging; however, it is difficult to evaluate bulging using the POSAS and other existing tools. We used a question about bulging that assessed the general opinions of the patients and observer, but it was not a tool with proven objectivity. To address this limitation, we considered using a more objective measurement method or tool, but it was practically impossible to measure bulging smaller than 1 mm, as much more precise measurements would be needed. Thus, no further measurements were obtained. Presently, various scar assessment scales are available, but none has been confirmed to be reliable, consistent, feasible, and valid at the same time. This is a common limitation of other similar studies dealing with scars.
As modern medicine is developing with the introduction of new surgical techniques, plastic surgeons may experience a sense of surgical omnipotence. The definitive solution for scar management is surgical correction. However, patients always want non-invasive and more rapid treatment. Considering this, we can provide better outcomes by using both TCA injection and subcision as the first-line treatment for post-traumatic acute trap-door deformity.