INTRODUCTION
Inverted nipple is defined as a state in which part of the nipple or the entire nipple is retracted below the surface of the areola. Inverted nipples can be classified in accordance with Han and HongŌĆÖs classification [1] as follows: grade I (mild), grade II (moderate), and grade III (severe).
Surgical correction aims to achieve aesthetically satisfactory nipple projection without recurrence, while also maintaining the sensory and lactation functions [2]. Various surgical methods have been suggested for correcting inverted nipples, including dermal and dermoglandular flaps, endoscopic release, internal suturing, continuous traction, and the use of artificial dermis [3-8]. The variety of surgical techniques reflects the difficulty of achieving a satisfactory outcome with any single method.
A surgical technique employing 2 horizontal mattress sutures was suggested by Gould et al. [9] in 2015. This is a relatively safe and effective method, but we found that the shape of the nipple base immediately after surgery was angular, and that satisfactory nipple projection was difficult to achieve with time; accordingly, we developed a new method, as described in this report. Using the surgical method of Gould et al. [9] as a benchmark, we surmised that combining this technique with purse-string suturing would produce a better outcome. Thus, we introduce a surgical technique that combines 2 suture-based methods.
IDEA
Surgical procedure
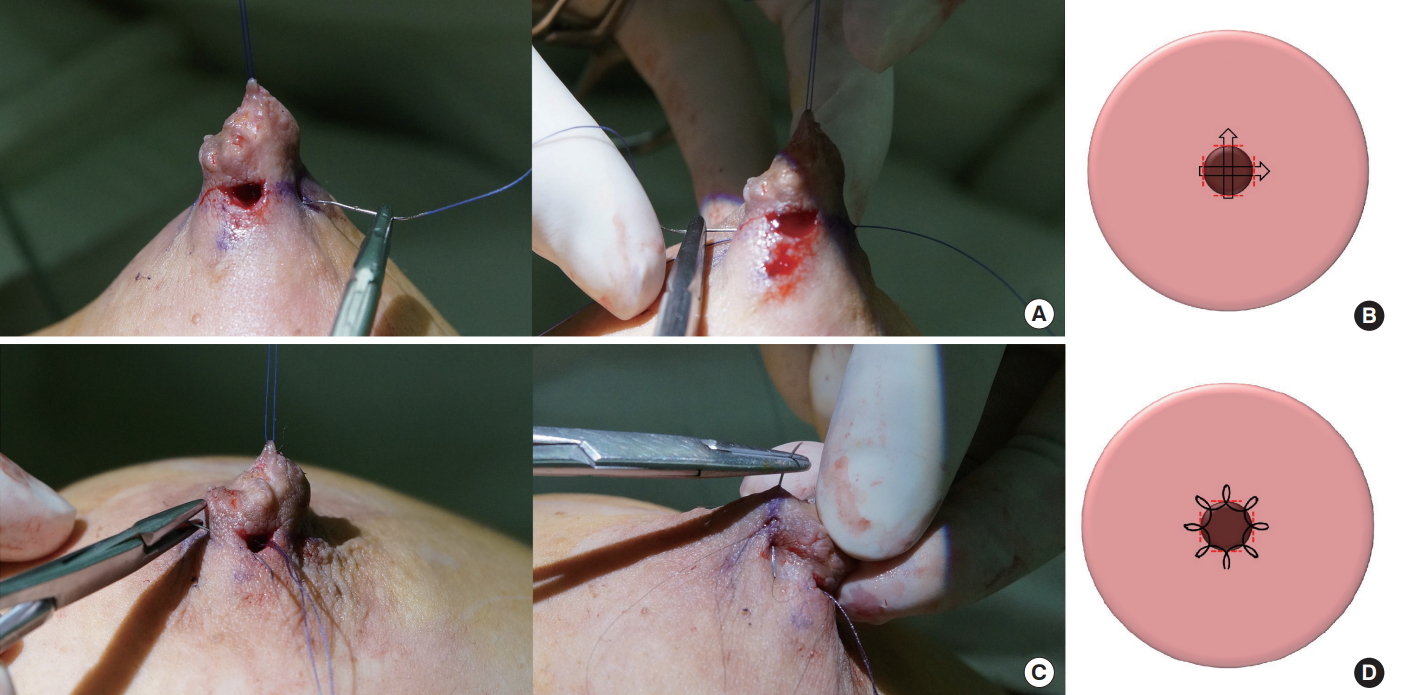
Gould et al. [9] proposed a surgical method for correcting inverted nipples in 2015. Four slit incisions are made in the nipple base (at the 3, 6, 9, and 12 oŌĆÖclock positions) while the patient is under local anesthesia, and the fibrotic band located at the nipple base is dissected and released. Next, 2 horizontal mattress sutures are performed in a perpendicular direction with 4-0 Vicryl (Fig. 1). We used the same method described above, but followed this with a purse-string suture without an additional incision, as in non-incisional double eyelidplasty or knifeless otoplasty. Starting from the slit incision at the 6 oŌĆÖclock position, a purse-string suture was placed around the nipple base with 7-0 nylon, followed by 8 stitch points at equal intervals.
The length of the skin incision for the horizontal mattress sutures must be limited to 3 to 5 mm, and no separate incision was made for the purse-string suture. When performing the purse-string suture, a needle was inserted back into the stitch points from which it came out, without a skin incision. The purse-string suture was ligated with proper tension, and the knot was buried beneath the dermis (Fig. 2). The skin incisions were then sutured with 7-0 nylon, antibiotic ointment was applied, gauze was loosely placed, and the wound was disinfected with a nipple protection cup. The temporary traction suture was not removed, but was tied to the nipple protection cup to maintain traction. This traction was removed after 3 to 5 days.
Case
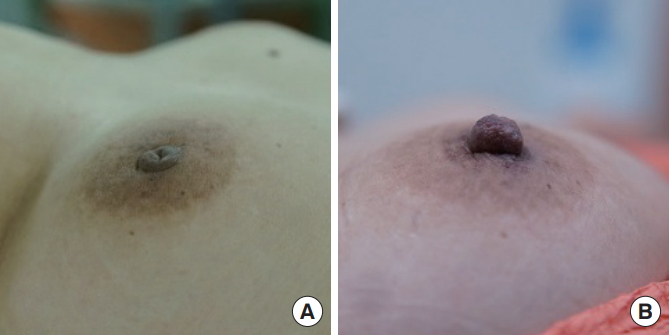
A 50-year-old woman underwent surgery for grade II inverted nipple in her right breast. The patient was monitored for 6 months postoperatively, during which time there were no adverse effects, such as hematoma, bleeding, nipple necrosis, or sensory loss (Fig. 3). The nipple was well maintained without any significant loss of projection after surgery, and the patient was satisfied with the surgical outcome.
DISCUSSION
The creation of lasting nipple projection remains a challenging problem in the correction of inverted nipples. Surgical techniques to correct inverted nipples have been studied, and various methods have been suggested, such as dermal and dermoglandular flaps, endoscopic release, internal suturing, continuous traction, and the use of artificial dermis [3-8,10]. Techniques using sutures have the advantage of reducing incisions and scarring, and are also considered safe. Perpendicular sutures, purse-string sutures, and continuous subcutaneous sutures have been used [11-14]. In particular, we thought that the surgical method published in 2015 by Gould et al. [9] was a safe and effective technique to correct inverted nipples. Therefore, we performed this technique on our patients, but in some cases the patients were not satisfied with the result. They complained of an angular nipple base immediately after surgery and gradual nipple projection loss. However, these patients did not agree for their clinical photographs to be used, meaning that unfortunately there are no clinical photographs in this article.
The technique described herein combines perpendicular absorbable sutures and purse-string non-absorbable sutures. Our surgical method involves first placing a pair of perpendicular sutures using a horizontal mattress suture technique with 4-0 absorbable materi al, followed by a purse-string suture with 7-0 non-absorbable material. The horizontal mattress sutures provide basic support for the maintenance of nipple projection immediately after surgery, and the purse-string suture provides additional strength to maintain projection. Use of a purse-string suture with non-absorbable material prevents the loss of projection with the gradual absorption of the horizontal mattress suture, in which an absorbable material is used. Moreover, the purse-string suture helps to form a nipple base with a more circular shape after surgery.
In the surgical technique presented in our study, 7-0 nylon is used for the purse-string suture, which is finer than the sutures used in previous methods, and only 8 stitches are needed [12,13]. The reduced number of stitches makes surgery simpler than other pursestring suture techniques, thereby reducing the duration of surgery. In addition, the finer thread should reduce the likelihood of the suture material being palpable or exposed after recovery. The strength needed to maintain the projection is reduced by the use of fewer stitches and finer thread, but is compensated for by the use of perpendicular sutures. Combining 2 suture techniques to maintain projection prevents excessive force on the purse-string suture, thereby reducing the risk of reduced blood supply to the nipple [13].
Inverted nipples still present a challenge for plastic surgeons. Our combined use of 2 different suture techniques to provide sustained nipple projection is simple, safe, and reliable. However, the follow-up duration in this study was relatively short, and additional long-term monitoring will be required.