INTRODUCTION
Aesthetic rhinoplasty procedures have increased in frequency in the Asian population. Although aesthetic concepts differ for each race, the current concept of nasal beauty shows a tendency to coincide with that of Caucasians. The ideal, beautiful nose tends to have a straight dorsum from the radix to the tip, with an adequate height. The tip should be slightly more prominent than the dorsum, and the columella must be of sufficient length to provide the necessary projection of the nasal tip above the dorsal line. The nasolabial angle should be between 90 and 110 degrees, and elliptical pear-shaped nostrils are preferred. Asians commonly desire aesthetic rhinoplasty because of a flat or low dorsum, acute nasolabial angle, poorly projected and caudally rotated tip, short columella, wide alar base, and a round or flared nostril shape [1-3]. Therefore, the surgical procedure mainly focuses on dorsal augmentation and tip projection [4]. The low nasion and dorsum can be augmented with various methods using autogenous or alloplastic materials. However, a bulbous nasal tip, wide alar base, acute nasolabial angle, and recessive pyriform fossae further compound the difficulties. The surgeon can manipulate the footplate area of the medial crus (which plays an important role in nasal tip projection, nasolabial angle, length of the columella, and nostril shape) to achieve the desired effect. In Asians, the length of the footplate segment is much longer than in Caucasians, and since Caucasians and Asians have anatomic differences in their nasal configurations, a different surgical approach would be needed for each of the different races.
In 2004, we reported on 110 consecutive Asian patients who underwent aesthetic rhinoplasty with the addition of a footplate incision to obtain greater satisfaction [5]. Nowadays we still perform the reported technique with several modifications. During the long term follow-up since publication of the article, no significant complications were reported and we still think that this method contributes to Asian Rhinoplasty. In this follow-up study, we report on our new cases and focus on a few changes.
METHODS
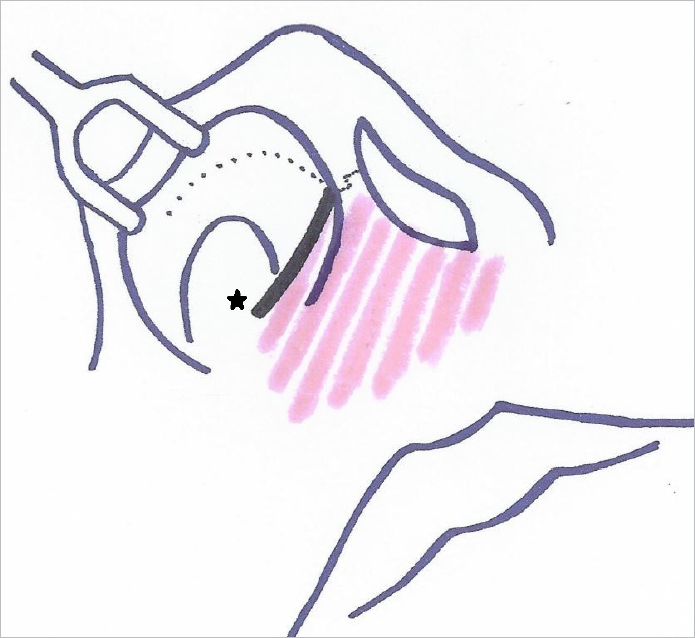
All procedures were performed under local anesthetic infiltration (1% lidocaine mixed with 1:200,000 epinephrine). In the endonasal approach, the incision followed the caudal border of the lateral crus, cephalad to a soft triangle at the nostril apex; then immediately continued adjacent to the caudal border of the medial and middle crura along the columella rim; and extended along the caudal border of the footplate of the medial crus onto the floor of the nasal vestibule bilaterally. In the open approach, a stair step transcolumellar incision was added (Fig. 1).
In this study, we emphasize a couple of recent changes in our procedure since the publication of the prior article. First, we excised the dog-ear that appeared at the caudal end of the extended footplate incision due to the projected tip. Second, the undermining of the inferior columellar area was subcutaneously carried out wider than before to obtain more tip projection and further improve the columello-labial angle. In the previous study, undermining was done just below the incision, namely around the columello-labial junction. But after modification, we widened the area of undermining to upper half of the upper lip. A pocket was then created in the nasal dorsum for implant insertion. A number of materials have been used for nasal augmentation, and the implant was fashioned and inserted into the dorsal subperiosteal pocket for dorsal augmentation and between the medial crura as the midcolumella strut.
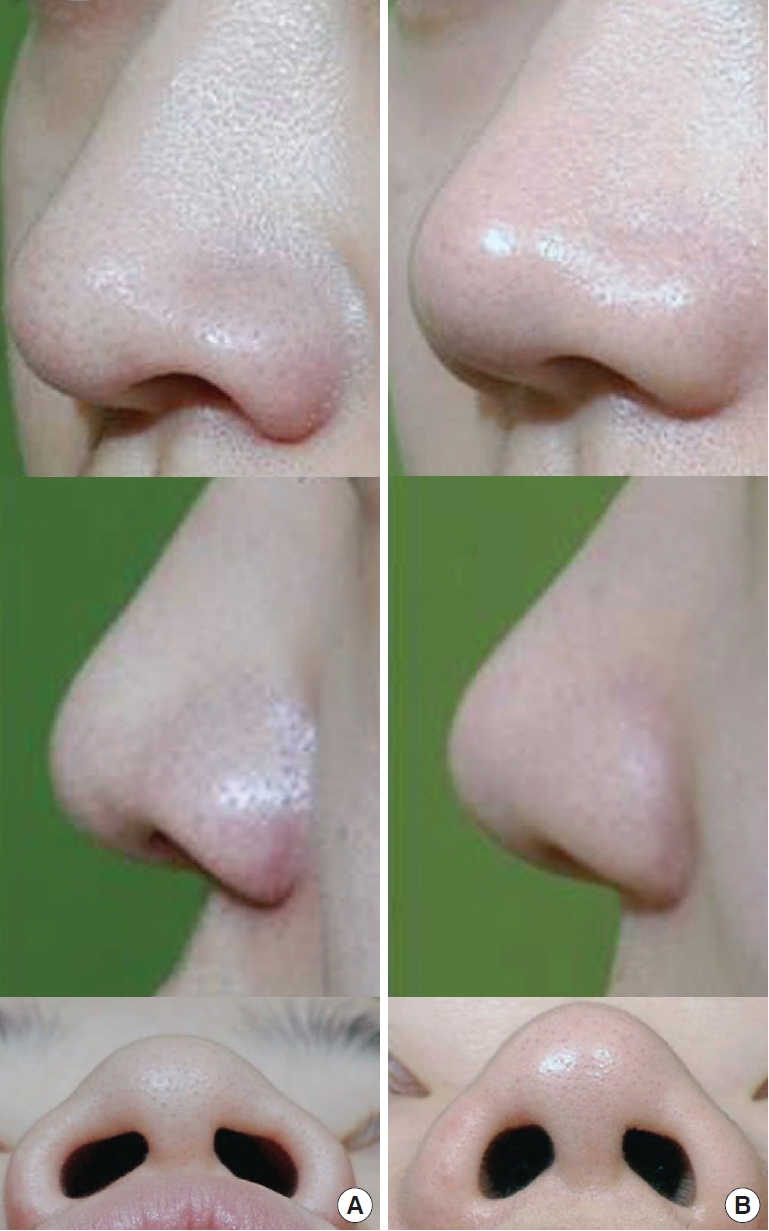
This study included 85 additional patients (32 male and 53 female) who underwent aesthetic rhinoplasty using this extended footplate incision from August of 2010 to May of 2013. The mean age was 29 years and ranged from 20 to 59 years. Sixty of these patients underwent endonasal rhinoplasty (Fig. 2 and 3), while 25 patients underwent open rhinoplasty (Fig. 4). Seventy-one cases consisted of primary rhinoplasties while 14 had had previous nasal augmentations. Cartilage work was done in every open rhinoplasty case and cartilage onlay graft was added in 18 cases. The postoperative results were evaluated for at least 12 months following the procedure. A total of 43 patients had an adequate follow-up time, with an average of 15 months. Finally, patient satisfaction and postoperative complications were recorded.
RESULTS
All patients showed an improvement in nasal height, tip projection, and nostril shape. The majority of the patients (40/43 cases; 96%) were satisfied with their nasal shape, and the three dissatisfied patients wanted further nose augmentation. Interestingly, 30% of the patients complained of an over rotated or over projected tip in the early postoperative period, but all of these patients became accustomed to and satisfied with their new nasal shape within 1 month of the procedure, even though the tip projection did not diminish. Two patients exhibited complications consisting of a mild nostril scar contracture, but this condition improved within 6 months postoperatively. Although a mild degree of asymmetry was noted in the nostril shapes of some patients, neither the patients nor the surgeons felt that it was clinically significant. There were no cases of implant extrusion, displacement, or infection. The extended footplate incision does not cause any problems because the scar is completely concealed. In addition, there were no respiratory complaints, and no revision procedures were performed.
DISCUSSION
In some surgical innovative ideas, major problems or complications were found during the long term observation. These may result in abandonment of that methods after publication but future surgeons may still experience same problems if it is not updated. Therefore, the main focus of this article was to identify the safety and emphasize the efficiency of this footplate incision after long term follow-up. During the 10-year of long term follow-up and newly added cases since publication of the previous article, no significant complications were reported and we still think that this method contributes to Asian Rhinoplasty.
The anatomy of the footplates plays an important role in nasal tip support and in nasal base structure [6]. The position of the footplates of the medial crura determines the dimension, the shape, and the projection of those structures, and any modification of the footplates may compel a change in the overall scheme of the rhinoplasty. Moreover, the shape of the nostril and the base of the columella are controlled. In Asians, the length of the footplate segment is much longer than that in Caucasians [7], and when operating on an Asian patient, a surgeon may be able to use a longer footplate segment to more effectively recreate the lower vault of the nose. As a result of these facts, we previously searched for procedures that would enable us to easily access the footplates of the medial crura. We therefore modified our footplate incision in both endonasal and open rhinoplasty to achieve a higher degree of satisfaction for aesthetic rhinoplasty in Asian patients.
The lateral curves of the medial crural footplates can be approximated to narrow and lengthen the columella. The columella was also caudally advanced, and thus the shape of the nostrils could be elongated. By simultaneously resecting the depressor septi muscle, significant rotation was possible in the cephalad tip. In addition, septal cartilage could be easily harvested without additional intercartilaginous and transfixion incisions. These manipulations might also be performed through a conventional open approach to rhinoplasty without our footplate incision. However, this incision requires only 2 more stitches and makes all of these procedures become much easier. More importantly, this simple additional incision can also allow further tip projection due to the reduction in pressure from the skin flap on the tip. To illustrate, extensive tip augmentation may result in the new nasal tip tilting upward too much or the tip implant may push the underlying alar cartilage dome downward as a result of the overlying skin flap pressure. With our footplate incision, more tissue can be borrowed from the lower columallar flap to reduce the overall pressure on the nasal tip. After making the new tip, a dog ear can be seen at the posterior end of the footplate incision. This indicates that further tip projection is created by the footplate incision. In the past, we left this dog ear because it can be naturally improved. However, some patients complained about this invisible lesion. Therefore, we modified our procedure to excise the dog-ear that appeared at the caudal end of the extended footplate incision. Since there is a natural limit to the amount of tip heightening possible, and since even a few millimeters can be most helpful, we believe that the footplate incision is very useful. In addition, wide undermining of the inferior columellar area is subcutaneously carried out to further improve the tip projection and columello-labial angle. In the previous study, undermining was done just below the incision, namely around the columello-labial junction. But after modification, we widened the area of undermining to upper half of the upper lip. Because Asians have thicker nose skin and overlying skin flap pressure is limitation of tip augmentation, reducing tension of inferior columellar flap by wide undermining is considerably helpful. We have recently had more success in correcting tip deformities by using this incision.
The endonasal approach is appropriate for select patients due to the lower chance of complications and shorter procedure time. Open rhinoplasty with a transcolumellar incision is a type of surgery that can be more easily controlled. However, an extended nasal tip edema and columellar scar is some of the disadvantages of using this method. An endonasal approach with an extended footplate incision allows a patient to avoid these disadvantages and provides a more controlled procedure, in a manner similar to the open method.
Implant extrusion or translucency is significant complications that result from dorsal and tip augmentation with silicone [3,8]. These conditions are mostly due to the overcorrection or high pressure of the overlying skin [9,10]. These complications have not yet been experienced with our extended footplate incision procedure with a sufficient follow-up time.
One limitation of this study is that there is no data comparing this incision with a control group. Because the purpose of this article is not reporting the superiority of this method, but reporting the safety, efficiency and technical refinement, we did not compare the result with the control group.
Any patient with an undesirable shape of the tip, nostril, columella, and nasolabial angle that requires access to the footplate of the medial crus can be considered as a candidate for this new incision. In addition, our extended footplate incision may be helpful when patients require a higher degree of tip projection and rotation. This technique may therefore be considered for use in primary or secondary cases.