INTRODUCTION
Skin covers the entire body. Skin texture is a very important factor from the perspective of beauty and anti-aging. To prevent or treat aging skin, it is important to focus upon the skin texture rather than volumizing effects in the subdermis, as the skin is the only organ that is visible. Thus, significantly improving a patientŌĆÖs skin texture after a face lift is critical, as neither skin texture nor dryness is improved by this type of surgery. Replacing the subdermal layer can improve wrinkles and skin folds by ballooning but do not improve skin texture or dryness.
A stabilized hyaluronic acid (S-HA) filler gel has been mainly used to treat folds and wrinkles associated with facial aging; S-HA has also been used as a filler that can be maintained for a longer time and yields better effects than other fillers [1]. Restylane Vital, one formulation S-HA, that is comprised of small particles [2], however, it is difficult to inject S-HA into the dermal layer without forming lumps on skin [3,4]. This is the major reason for the development of the present method, which uses a mesogun injector that is able to divide 1 cc S-HA into 1,000 microdroplet injections.
Previous studies and manuals from manufacturers describe the optimal volume of the S-HA injection method into the dermis as 0.02 cc or 0.025 cc [2,5-8]. Moreover, they state that the injection depth would correspond with the dermis, while it is actually the subdermis [2,5-8]. In this regard, the refined method of S-HA injections will be described.
METHODS
The study was a single-center, prospective, in vivo study with dermal and subdermal injections of particle type S-HA gel (Restylane Vital; Galderma, Uppsala, Sweden). Informed consent was obtained from each patient, and the study adhered to the tenets of the Declaration of Helsinki. The dermis was injected using an injector (DermaQueen; Woorhi Medical, Seoul, Korea or Vital Injector; Eunsung Medical, Seoul, Korea). Some patients had subdermal injections after 1 year to compare different effects of different injection depths for an intra-individual comparison.
Patients
A total of 150 patients (135 females, 15 males), with an average age of 51.2 years, participated in the study. The injection areas included the following: dry facial skin (100 patients), dry dorsal hand skin (30 patients, dry elbow skin (5 patients), dry leg skin (5 patients), dry hip skin (5 patients), and oily skin with large skin pores and acne scars (5 patients).
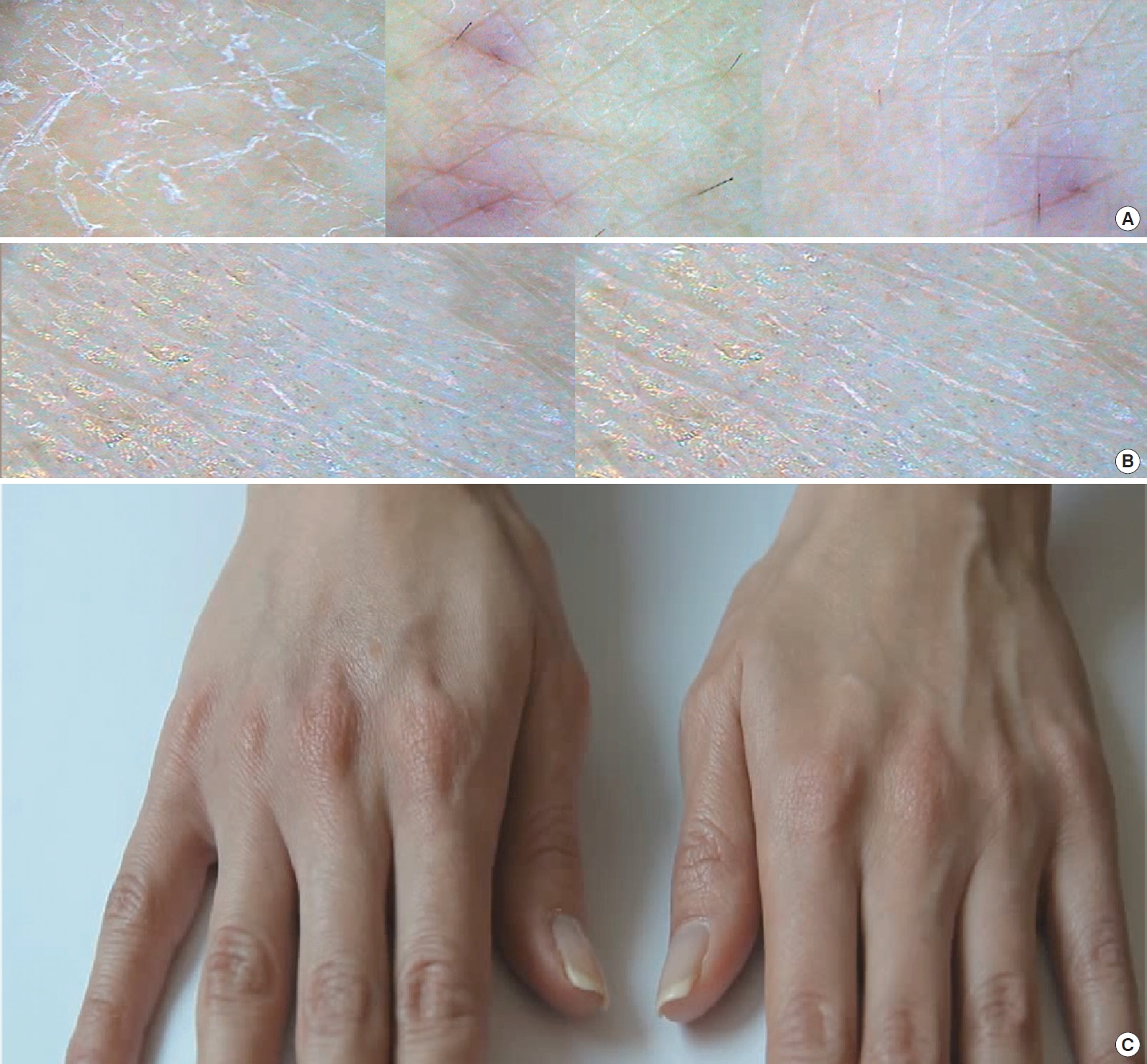
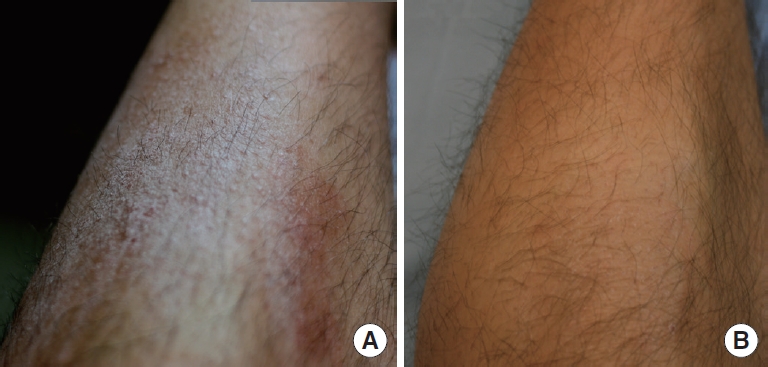
From December, 2009 to December 2012, patients with subjective signs of dryness on the face, back of the hands, elbows, legs, and hips participated in the study. They were also concerned about the visible signs of large skin pores and acne scars. Additionally, subdermal injections were performed on the same patients after 1 year to compare the effects on the face and hands for an intra-individual study (Fig. 1).
Injection method
Before the treatment, a 9% lidocaine topical anesthetic cream was applied to the injection area and covered with plastic wrap for 40 minutes.
Patients were injected with 1 cc Restylane Vital that was divided into 1,000 shots using the injector (DermaQueen or Vital Injector). This device has five needles and the distribution of the microdroplet injections provided a more regular distance than manual injection. Particle type S-HA (Restylane Vital) was injected into the dermis for longevity. The injection depth was controlled by a touch panel on the injector (0 to 2 mm). Injection depth in this study was about 1 mm on monitor of injector. But there was bevel in tip of needle, actual depth of injection was less than 1 mm. During this procedure, the injection depth was reduced if substantial bleeding was noted, as indicated that the injection penetrated the subdermal plexus. After the injections, cold compression was performed to spread the S-HA and to reduce pain and ecchymosis. In thin skin, such as the lower eyelid, lumps can be made easily and it is hard to spread lumps several weeks after the injections.
Measurement of biophysical parameters
Biophysical measurements were obtained without lotion or any skin products. The patients remained in a comfortable emotional state for 30 minutes before taking the measurements to avoid confounding results.
Skin roughness and morphology
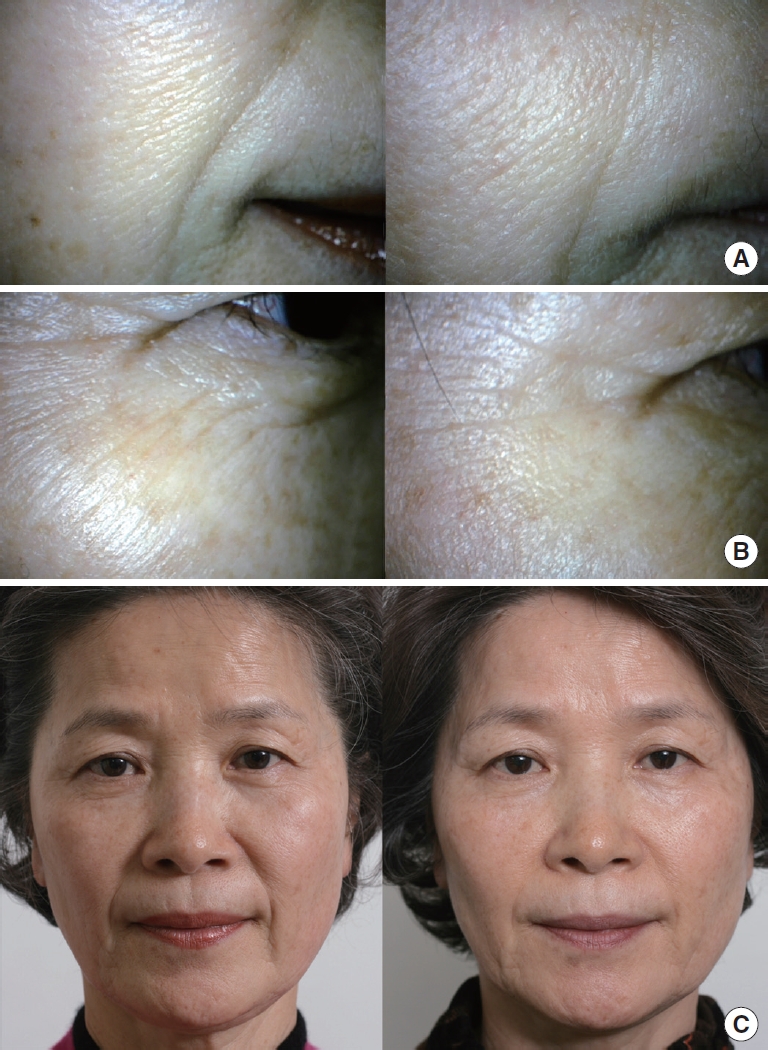
Skin roughness and morphology were evaluated using a standard, non-contact method with a dermatoscope (├Ś50, ├Ś100, and ├Ś200 resolutions, Coscam, Sometech, Korea) (Fig. 2). A microscopic view of skin roughness was evaluated subjectively, using five levels: 1: very rough, 2: rough, 3: moderate, 4: smooth, and 5: very smooth. Measurements of skin roughness were carried out prior to the first treatment (baseline, week 0), and at 1, 2, 6, 12, and 24 months after treatment (only a few patients were followed for 2 years). To ensure that the measurements were taken at the exact treatment area, landmarks were included in the image: moles, lip corners, vessels, and scratch marks.
Dermal hydration
Hydration of the dermis was measured using a digital multimeter (digital multimeter model 1009; Kyoritsu electrical instrument works, Tokyo, Japan) with two 31 G needle to penetrate the epidermis. Two 30 G needles were glued to a simple measuring apparatus, and the distance between the needle tips was 2 mm. Using individual simple needles, dermal electric resistance was checked by a current of 0.4 mA before treatment and 4 weeks after the procedure. In addition, skin dryness was evaluated subjectively by the patient using five different levels: 1: very dry, 2: dry, 3: moderate, 4: hydrated, and 5: well hydrated.
Dermal thickness
Dermal thickness of the hand and face was checked by ultrasonic imaging (Medison, Seoul, Korea) before and 4 weeks after the procedure. The thickness of the hand was checked at the middle of the second metacarpal bone, and the thickness of the face was checked at the center of a line from the epicantus to the mouth corner. To prevent compression errors, the ultrasound probe was applied lightly as possible.
Biopsy
Biopsy was carried out in some volunteers to confirm the depth of the injections and to observe the S-HA particles in the dermis after 2 weeks and 12 months. The depth of the injections of S-HA and tissue reactions, such as foreign body reactions, fibroblasts, and new collagen synthesis, were observed by biopsy.
RESULTS
Skin roughness and morphology
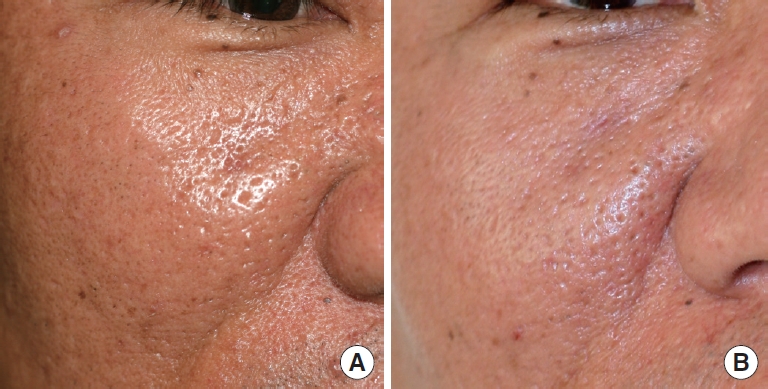
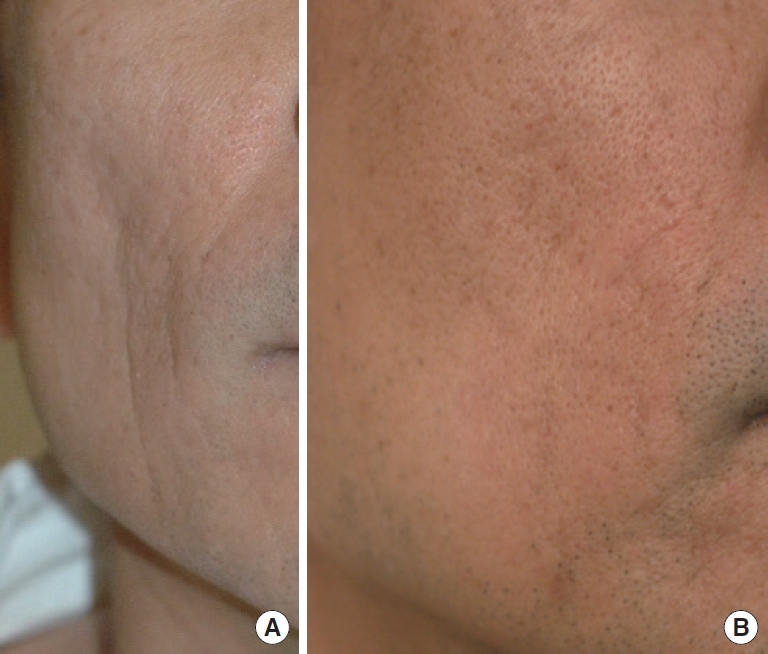
Skin roughness was improved by 1.83 points (from 1.34 to 3.17) under microscopy (├Ś50) after 4 weeks (Fig. 2, 3, Table 1). Subjective skin roughness was improved by 1.27 points (from 1.45 to 2.72) after 4 weeks (Fig. 4). Large skin pores were reduced after intradermal injections with particle type S-HA (Fig. 5). Nasolabial folds and fine wrinkles in thick skin were also improved (Fig. 2, 4, and 6).
Microscopic changes were more frequently observed than macroscopic changes. Some patients who had significant changes on a microscopic level had no recognizable improvements at earlier times. There were fewer skin texture changes microscopically in cases of subdermal injections of S-HA on the face and hands (Fig. 1).
Dermal hydration
Subjectively, dryness was improved 2.54 points from 1.28 to 3.82. Hydration of the dermis changed after 4 weeks. Subjectively, dry skin was satisfactorily treated with S-HA (Fig. 7). The electrical resistance of the dermis decreased after 4 weeks without statistical significance (23.07 M╬® to 12.24 M╬®).
Dermal thickness
Dermal thickness of hands was increased by 4.2% (1.19 to 1.24 mm) 4 weeks after the injections. There were no significant changes in dermal thickness in cases of subdermal injections in the dorsal hand. There were also fewer changes in skin texture microscopically in cases of subdermal injection (Fig. 1).
Biopsy
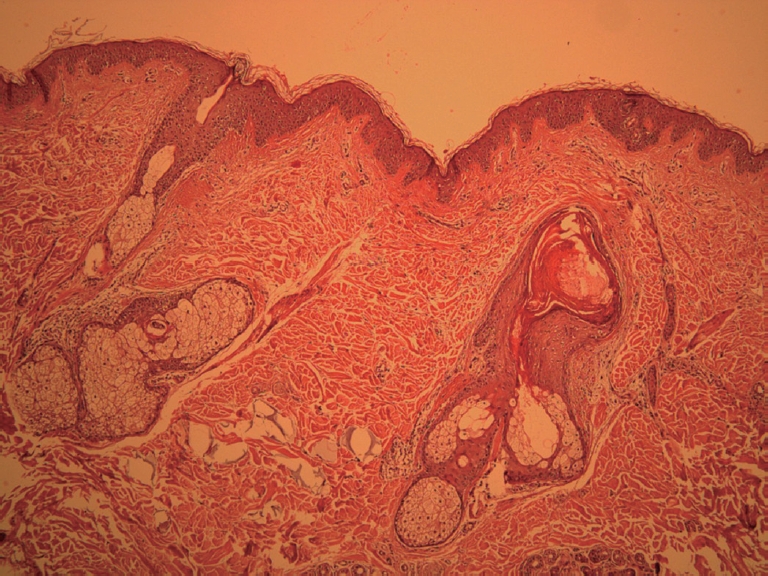
The particle size of Restylane Vital in the dermis was 100 to 150 microns in the biopsy study. Filler gels were found in the dermal layer which occupied most of the dermis (Fig. 8).
Collagen fibers were displaced by particles of S-HA and there was a higher density of collagen around the S-HA microdroplets. Collagen bundles stained blue with MassonŌĆÖs trichrome stain. Few new collagen fibers were found around the microdroplets after 2 weeks, whereas more new collagen was found after 12 months. Some new collagen is synthesized by stretching fibroblasts according to reports of Wang et al. [10] and Tran et al. [4] There were no foreign body or tissue reactions (Fig. 8).
DISCUSSION
In previous studies of S-HA injection, many authors have misunderstood injection depths and volumes. S-HA at a volume of 0.02 cc per injection can make lumps in the dermis, but monophasic S-HA does not. Monophasic S-HA can spread more than 10 mm, but particle type S-HA does not, because it is comprised of relatively large particles of S-HA. For example, Restylane Vital is comprised of 100 to 150-micron particles. For these reasons, dermal injection should be differentiated between particle type S-HA and other monophasic S-HA formulations like Esthelis (Anteis, Geneva, Switzerland), Juvederm (Allergan, CA, USA), and Teosyal (Teoxane, Geneva, Switzerland). Monophasic fillers can be used at variable volumes without a risk for lump formation, because they spread out well [3,4].
Dermal injections cannot cause hematomas; real skin rejuvenation occurs when the injection is done into the dermis. The blood vessels that cause hematomas are located in the dorsal intermediate lamina. If the injections are performed into the dermal layer, patients should not experience hematomas, but petechiae or ecchymosis may still occur.
Williams et al. injected 0.025 cc per particle type S-HA injection into the hand with a distance between injection sites of more than 2 cm [2]. These authors described that the skin texture was improved after injection into the dorsal superficial or intermediate lamina. Particle type S-HA improved subdermal volume but skin texture was not changed after deep injection. The results of injection appear to depend on injection depth, that is, ŌĆ£a different depth creates different results.ŌĆØ
Even manufacturers instruct to inject into the dermal layer with a blunt needle (PixelŌĆÖ cannula). And S-HA was injected using blunt micro-cannula for ŌĆ£skinboostersŌĆØ [9]. In fact, it is impossible to inject the dermal layer with a blunt needle (cannula). This erroneous concept about depth might cause unwanted results.
If clinicians want to improve skin texture, a more superficial injection will achieve this goal. Deeper injection or subdermal injection can only augment in the volume of the subdermis. The purpose of particle type S-HA is to improve skin rejuvenation and hydration, not volume. Real skin rejuvenation can be achieved when injections into the dermis are made. Particle type S-HA injection into the subdermis can expand skin, making the surface look tighter. Subdermal injection is also effective for improving fine wrinkles. Sometimes, these two types of injection can cause similar results for thin skin, especially in Caucasians. However, since Asian skin is thick, subdermal injections with S-HA cannot change skin texture. In this regard, the aforementioned ŌĆ£re-teenage methodŌĆØ could be effective for many Asian doctors.
ManufacturersŌĆÖ guidelines recommend three injections every month. However, particle type S-HA lasts more than 18 months; frequent injections may be suitable for monophasic S-HA but not for particle type S-HA [4]. Distante et al. [5] used S-HA to rejuvenate the skin of the upper arm, with three sessions at 30-day intervals. They injected 0.03 cc per injection, with sites 1.5 to 2.0 cm apart, into the mid to deep dermis, but that must have made lumps in the dermis of the arm, even though this effect was never mentioned in the study.
In the biopsy study, monophasic S-HA did not last longer than biphasic S-HA. This injection method with particle type S-HA using a mesogun was named ŌĆ£Re-teenage,ŌĆØ which means ŌĆ£to return to the teenage yearsŌĆØ so as to distinguish it from monophasic S-HA. To improve either the dermis or skin texture, more superficial, biphasic S-HA is a better choice. Meanwhile, superficial injections of particle type S-HA have a higher risk of lumps than monophasic S-HA. Using this injection technique for dry skin, fine wrinkles and skin roughness can be successfully treated for more than 1 year.
CONCLUSION
Particle type S-HA can improve skin texture and skin roughness. For dermal hydration, particle type S-HA can be used, and for soft tissue augmentation, subdermal injection of particle type S-HA can be used. Clinicians can inject particle type S-HA into the dermal layer with small volumes (about 0.001 cc, 1 ┬ĄL) using a mesogun.