INTRODUCTION
Periorbital hyperpigmentation (POH), generally called “dark circle,” is a condition characterized by relatively dark coloration of the periorbital eyelids. It is a common worldwide problem, which makes a person appear tired, sad, and aged. Although this condition does not cause physical morbidity, it can pose a substantial cosmetic problem and, eventually, affect the quality of life of the effected individual.
A number of factors can cause dark circles around the eyes. One cause is excessive pigmentation due to dermal melanocytosis. This can be congenital or occur secondary to such conditions as atopic or allergic contact dermatitis [1]. Another common cause of dark circle is a thin, translucent lower eyelid skin overlying the orbicularis oculi muscle. Transparent eyelid skin allows visualization of the underlying subcutaneous vascular plexus or vasculature within the muscle [2]. Shadowing due to skin laxity and tear trough is another cause of infraorbital dark circle [3]. This can worsen with time because of age-related loss of subcutaneous fat and hollowness of the periorbital area.
Therapeutic modalities for dark circles differ depending on the primary causative factor. Although a number of treatment options are available, autologous fat transplantation is known to be effective, especially for patients with the vascular type of dark circle [4]. Injecting fat between the skin and muscle can be expected to act as a barrier that prevents visualization of hypervascularity within the muscle. One of possible complications of autologous fat grafting is the irregularity caused by visible lumps. We have encountered several complicated cases of lumped fat, which required removing the fat through an infraciliary incision.
In 2013, Tonnard et al. described a nanofat grafting technique [5]. These authors applied a mechanical emulsification process to achieve much finer fat particles. In contrast to the typical fat grafting method, which acts primarily by producing a physical volume effect, nanofat grafting may act primarily by the activity of transplanted stem cells.
The purpose of this study is to evaluate the effectiveness of the nanofat grafting technique in correcting infraorbital dark circles.
METHODS
Patients
Nineteen patients with dark circles due to increased vascularity and translucency of the skin were included. They underwent nanofat grafting for dark lower eyelids from December 2013 to March 2014 at a single clinic. Microfat grafting of the nasojugal fold was performed simultaneously in all patients. Eighteen patients also underwent transconjunctival fat removal during the same operation. The patients included 1 man and 18 women, aged 22 to 41 years old (mean, 30 years old). The mean follow-up period was 2.5 months, ranging from 2 to 4 months.
Operation methods
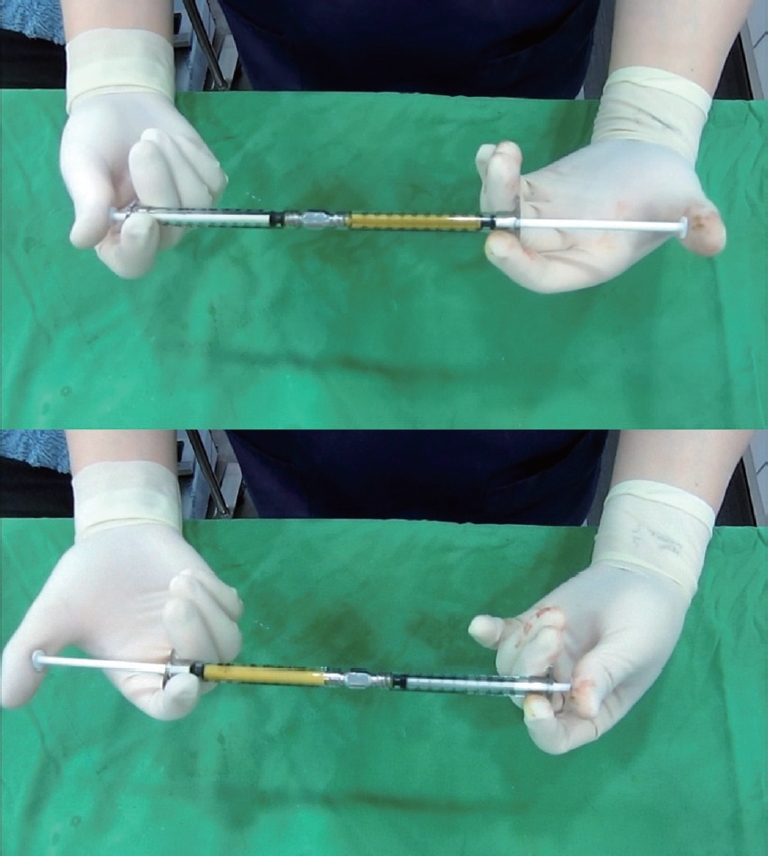
Fat was aspirated from the medial thigh or lower abdomen using the Coleman method. After centrifugation at 3,000 rpm for 3 minutes, the lipoaspirate was mechanically emulsified. Emulsification of the fat was achieved by shifting the fat between two 1-mL syringes connected to each other by a female-to-female Luer-Lock connector (Fig. 1). This differs from the technique introduced by Tonnard et al., in which 10-mL syringes were used [5]. After more than 30 transfers between syringes, the fat changed into an emulsion. To determine whether the fat was ready to inject, we used a 20 gauge blunt cannula, mounted into a 1-mL syringe. If there was no resistance when we gently pushed the piston of the 1-mL syringe, the emulsification process was deemed complete. Otherwise, we performed 30 to 50 more transfers and repeated the determination procedure. The emulsified fatty liquid was filtered over the sterile nylon cloth and the effluent was collected in a sterile recipient syringes.
First, microfat grafting was performed in part of the nasojugal groove. This was followed by nanofat grafting toward the upper part of the groove. The nanofat grafts were injected into the subdermal layer using a 20-gauge blunt cannula, inserted through a small incision approximately 2 cm below the lateral canthus. Injection continued until a smooth contour with the microfat-grafted area was achieved. The mean volume of microfat graft for each eyelid was 1.6 mL (range, 0.5–3.3 mL).
Assessment of outcomes
Standardized photographs were taken at baseline and at 2 months after treatment. All patients were clinically evaluated using these serial photographs by 10 plastic surgeons, who were blinded to the type of procedure performed. The improvement in pigmentation and skin texture was assessed using a grading scale: 0, <25% improvement (poor); 1, 26–50% improvement (fair); 2, 51–75% improvement (good); 3, 75–90% improvement (excellent); and 4, 91–100% improvement (complete). Patients also assessed their satisfaction on a quartile scale: 0, not satisfied at all; 1, slightly satisfied; 2, moderately satisfied; and 3, very satisfied. Postoperative complications, including ecchymosis, pain, edema, and erythema, were evaluated during the follow-up period.
RESULTS
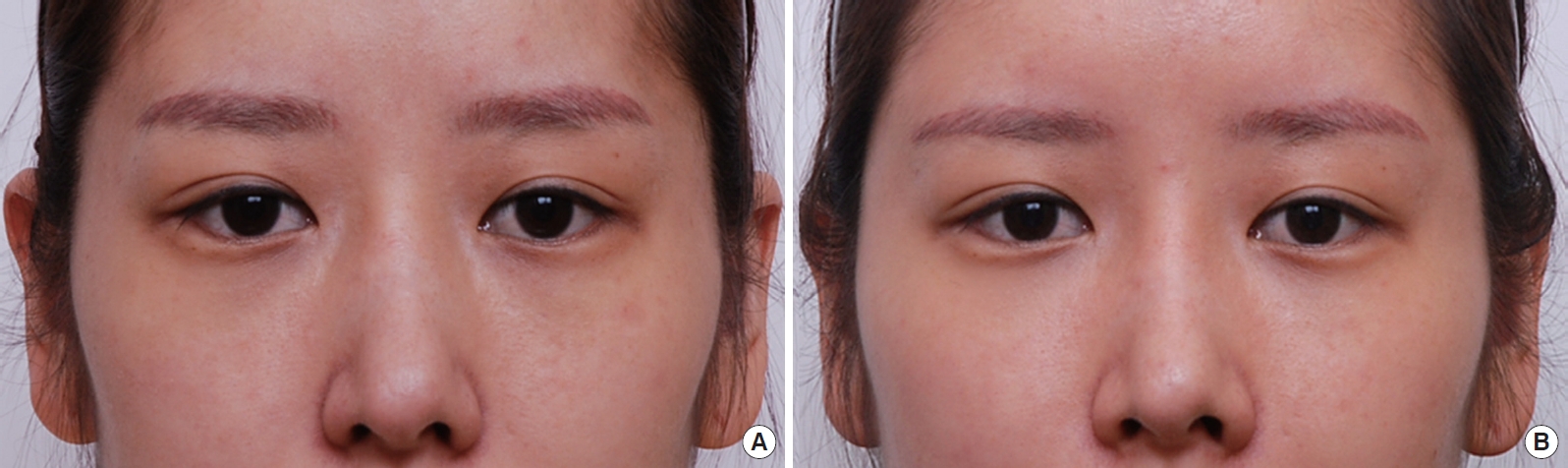
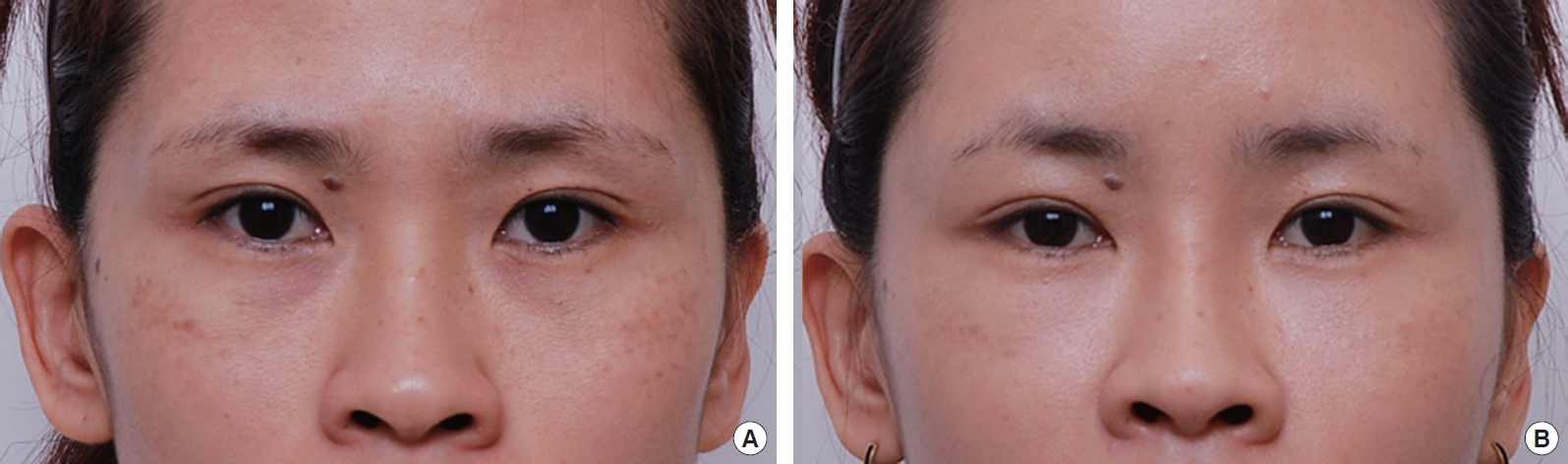
All patients were evaluated for improvement using photographic evidence and all showed much improvement from their preoperative degree of dark coloration. The patients exhibited a mean improvement of 70% (mean grading scale, 2.4) for physician objective improvement scores. Most patients exhibited improvement in the infraorbital darkening and skin texture of the lower eyelids (Fig. 2-5). However, none of the patients showed 100% improvement, which suggests that multiple factors contributed to the infraorbital dark circles and absorption of the injected nanofat. Most patients were satisfied with their improvement. The mean patient satisfaction score was 2.0 (moderately satisfied). There were no visible lumps of fat, contour irregularities, or fat necrosis. Postoperative erythema, pain, edema, and ecchymosis were minimal and rarely persisted for more than 72 hours.
DISCUSSION
Infraorbital dark circles affect individuals of both sexes, all races, and a wide range of ages. The condition causes considerable cosmetic concern and negatively impacts emotional well-being. Several factors are known to cause dark circles, including excessive pigmentation of the skin, thin and translucent lower eyelid skin overlying the orbicularis oculi muscle, and shadowing due to skin laxity and tear trough.
The most appropriate treatment modality differs depending on the main causative factor of the dark circle. Topical skin lightening agents are the mainstay of the treatment for hyperpigmentation. Agents commonly used for hyperpigmentation include hydroquinone, retinoic acid, mequinol, azelaic acid, and corticosteroids. Various combination therapies of these topical agents have been used to increase their efficacy while reducing side effects [6]. Chemical peeling, a process of removing the epidermis or upper dermis with chemical agents, is another option for patients with hyperpigmentation [7,8]. Lasers are also appropriate options, not only for hyperpigmentation but also for skin resurfacing [3,9,10]. Skin resurfacing with lasers is indicated for dark circles due to skin laxity and tear trough. Lasers used this purpose include the pulsed dye laser, diode laser, and 1,064-nm and 1,320-nm Nd:YAG lasers [2].
However, the aforementioned modalities are not effective for patients with dark circles due to thin, translucent skin. For patients with this type of dark circle, autologous fat transplantation has been reported as an effective method [4]. The vascular type of dark circle, due to a combination of transparency of the overlying skin and dense dermal vascularity, is the most common form of dark circle in Asian patients [10]. This may explain why topical agents, such as steroid or skin lightening creams, frequently fail to treat dark circles in this ethnic group.
For patients with light-colored, thin skin, soft tissue filler can be considered as an alternative treatment option, as the effect of autologous fat transplantation arises at least partially from the tissue acting as a barrier to reduce the translucency of the thin skin. However, soft tissue fillers have been reported to cause complications, including worsened pigmentation, a bluish color change, and increased vascularity. Lumps or contour irregularities are also common complications of soft tissue fillers, especially for thin eyelid skin. Goldberg and Fiaschetti reported that patients who were unhappy with soft tissue filler injection to the periorbital area tended to have thinner skin, which is more vulnerable to developing increased vascularity, bruising, or contour irregularities [11]. This is why fat grafting, which is readily available, safe, and completely biocompatible, is preferred to soft tissue fillers for dark circles accompanying thin eyelid skin.
According to Tonnard’s study, mechanically processing fat when producing nanofat completely disrupts the adipose tissue structure [5]. Thus, grafting with nanofat usually does not have a prominent direct volume-adding effect. Instead, the major effect of nanofat injection appears to relate to stem cell activity.
In the current study, nanofat grafting combined with microfat grafting produced satisfactory results in treating lower eyelid dark circles. Microfat grafting at the nasojugal folds compensated for the lack of volumetric effects of the nanofat grafting technique, and nanofat grafting at the lower eyelids improved the dark circles effectively, without any noticeable irregularity. This technique produces effects that are similar to those achieved by injecting purified stromal vascular fraction, but without the complicated technique or expensive laboratory equipment required for the latter. As well, the skin rejuvenating effects from stem cell activity are augmented by the fat graft acting as a soft tissue filler, to produce the final effect.
The nanofat grafting technique introduced by Tonnard uses very thin injection needles. Although there have been many studies of microfat grafting techniques using thin cannulas, Tonnard et al. used even thinner needles, as small as 27 gauge [5]. By contrast, we used a blunt cannula instead of a sharp injecting needle. In Tonnard’s cases, whitish discoloration remained for 1 month postoperatively and eyelid skin was erythematous for 3 months after the procedure. We considered these recovery times to be too long for actual clinical cases, so we decided to avoid intradermal needle injections.
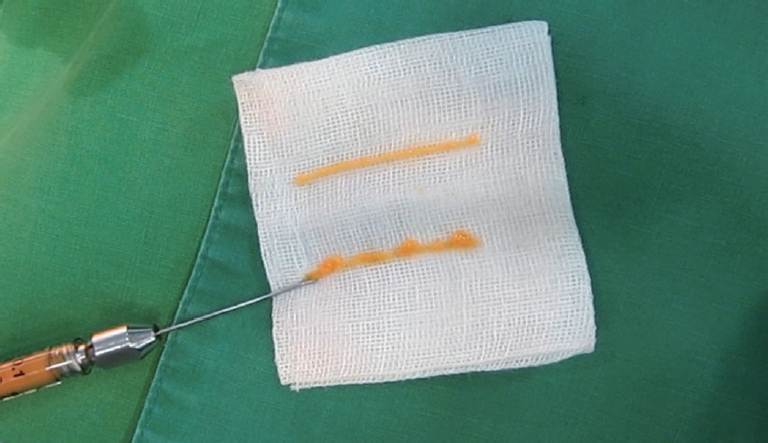
Although injected with a blunt cannula, the advantage of nanofat was apparent during the transferring procedure. In a mock injection, mechanically processed nanofat produced more regular and finer particles of fat than microfat using the same cannula (Fig. 6). In our practice, we have had patients with visible lumps following microfat grafting in the lower eyelids, which required removal of the grafted fat through an infraciliary incision in some cases. However, we have never observed irregularities using the nanofat technique.
Our final results were satisfactory, but we cannot be sure that they were as good as those produced by Tonnard et al. [5]. It is possible that better results could be obtained if the procedures included intradermal fat injection. However, we can expect the volume augmentation effect minutely comparing to Tonnard’s nanofat grafting. Further studies including histological examination may help address this issue.
In conclusion, for patients with dark circles due to thin, translucent eyelid skin, our nanofat grafting technique provided substantial improvements. Unlike microfat grafting, which is complicated in some cases by postoperative irregularities of the eyelid skin, nanofat grafting rarely causes complications such as lumps or irregularities. Our results suggest that the stem cell activity of the nanofat grafting technique has great potential as a treatment modality for skin rejuvenation in general, not only for the treatment of dark circles. This simple, cost effective procedure seems to be suitable for the correction of dark circles, and with further studies, nanofat technology will likely expand the indications for fat grafting techniques.