INTRODUCTION
The demand for facelifts is rapidly increasing in Asia because of economic development as well as the aging of the population. It is difficult to achieve satisfactory results, because of the facial characteristics of Asians. The goal of the facelift is to improve facial sagging. During initial stages, facelifts focused on the lower face. Various approaches, such as the extended superficial musculoaponeurotic system (SMAS) facelift, the finger-assisted malar fat elevation (FAME) facelift, and the high SMAS facelift, were designed to improve facial sagging in the mid- and lower face with the development of advanced facial surgical procedures [1-5]. Retaining ligaments is important for facelifts and was described by Furnas in 1989, because these ligaments support the soft tissue in its normal anatomical position and resist gravitational effects [6]. These structures attach the dermis, SMAS, and subcutaneous tissues to deep structures such as underlying muscle, bone, and parotid glands. There are two ligament systems. The first comprises true osteocutaneous ligaments: the orbital, zygomatic, and mandibular ligaments. The second involves tethering structures that do not originate from bone but attach the SMAS layer to the deep fascia: the parotid cutaneous and masseteric cutaneous ligaments. With aging, attenuation of retaining ligaments leads to the gravitational descent of subcutaneous fat and skin [7,8]. Also with aging, the tethering effect of retaining ligaments leads to deepening grooves, such as the nasojugal groove, nasolabial fold, and jowls [8,9]. We discuss facelift methods and retaining ligaments from an Asian viewpoint.
History of the facelift
Previously, facelift procedures were limited to skin excision. After methods of continuous incision, subcutaneous face and neck undermining, redraping, and excision of excess skin were recommended, establishing the principles of the facelift [10,11]. However, these conventional facelift procedures faced limitations that included aging and effects of gravity on the underlying structures. Dissection of the superficial fascial layer, which is connected to the platysma, was described by Skoog [12] Mitz and Peyronie developed the limits of the SMAS in the face and reported the advantages of SMAS tightening [13]. Subsequently, surgical procedures involving the deeper layers, such as the SMAS-platysma, were considered essential parts of the facelift. Various techniques involving the SMAS and platysma have been developed to improve outcomes. Midface and lower cheek lifts have received increased attention, because the midface is one of the most important facial structures [14].
Extended SMAS facelift
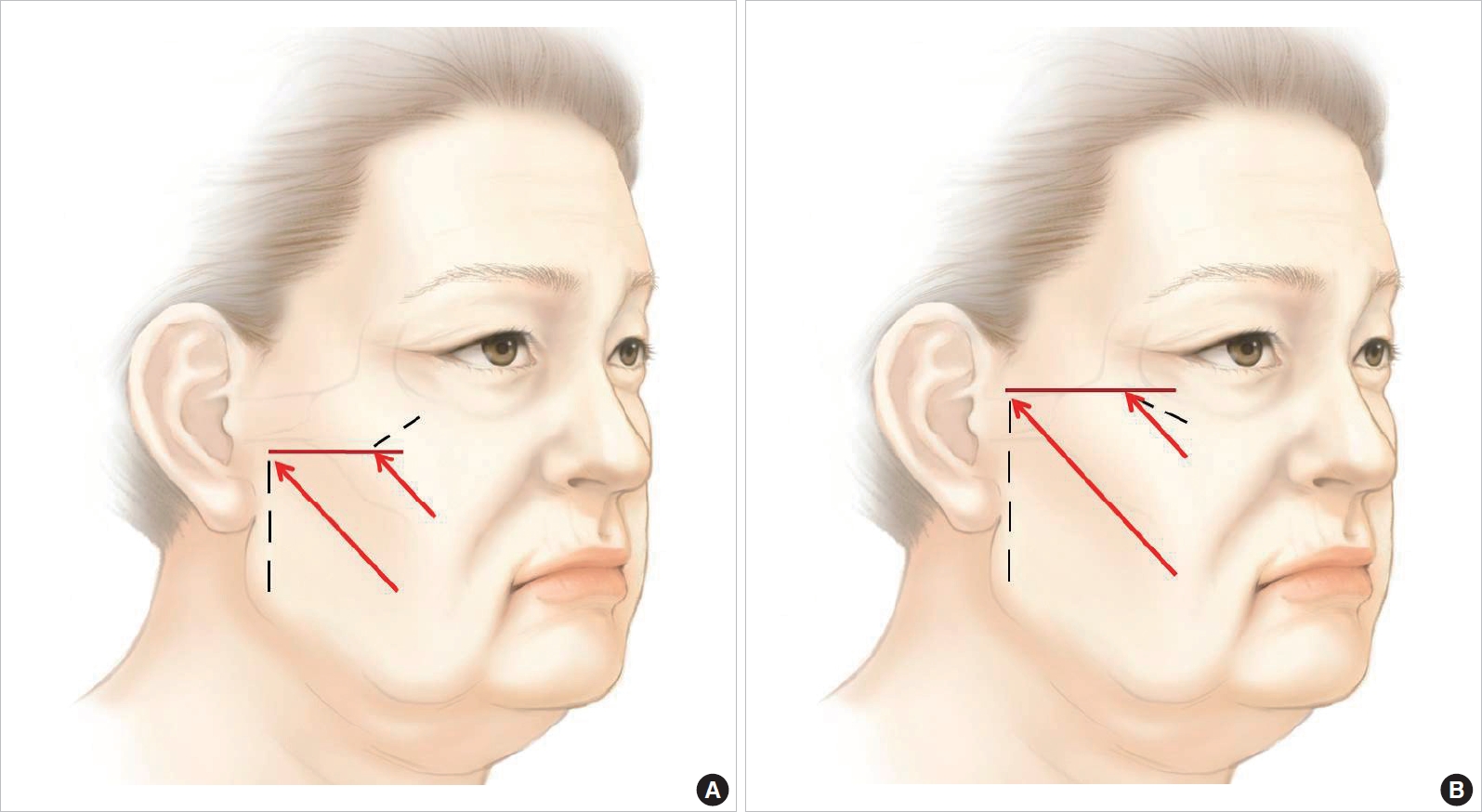
Basic techniques for the extended SMAS facelift are similar to traditional SMAS facelift techniques. With aging, dermal elastosis and skin laxity in the face do not occur in the same direction as the descending fat. These techniques then allow the raising of the dissected subcutaneous flap separate from the dissected SMAS flap, and these two layers can then be repositioned along two different vectors, [15,16] with minimal tension on the skin closure [17]. However, the extended SMAS facelift involves a more extensive dissection that releases the zygomatic and upper masseteric retaining ligaments in the sub-SMAS plane, improving facial sagging in the mid- and lower face (Fig. 1) [1,2]. This is a historically meaningful method because it released the retaining ligaments during a facelift for the first time. Extended dissection of the retaining ligaments allows for the free movement of the SMAS layer. An extended SMAS facelift can reposition the malar fat pad and improve the nasolabial fold and jowls [18]. This is an extremely effective procedure in Asians, in whom it is difficult to achieve satisfactory facelift results. However, it may be insufficient to improve sagging of the midface due to SMAS elevation and fixation below the zygomatic arch. The key fixation point is the preauricular area, as it is less effective in correcting facial sagging in the midface than is SMAS fixation above the upper border of the zygomatic arch (Fig. 2).
Facelift using the FAME technique
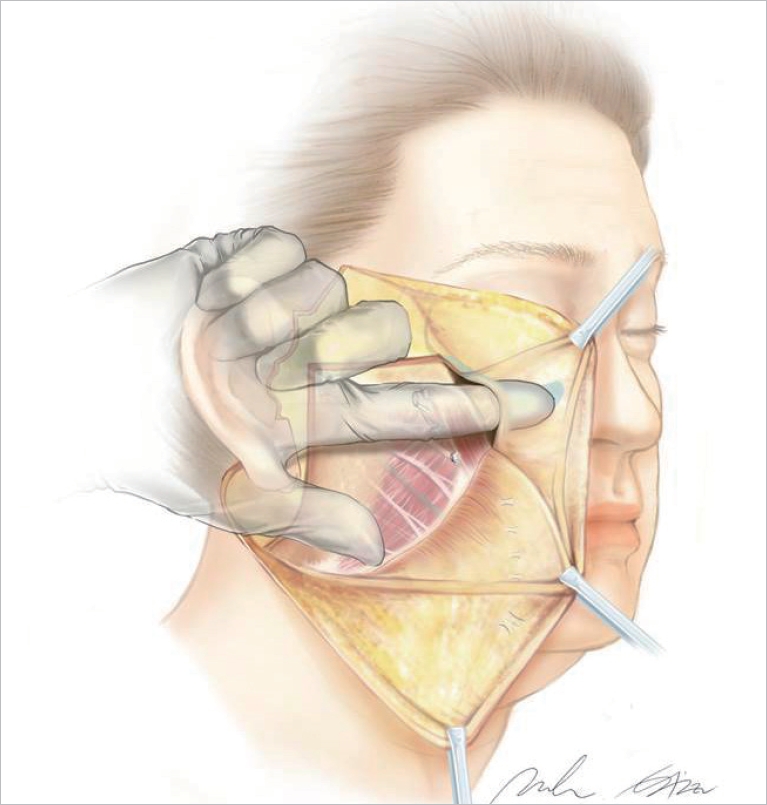
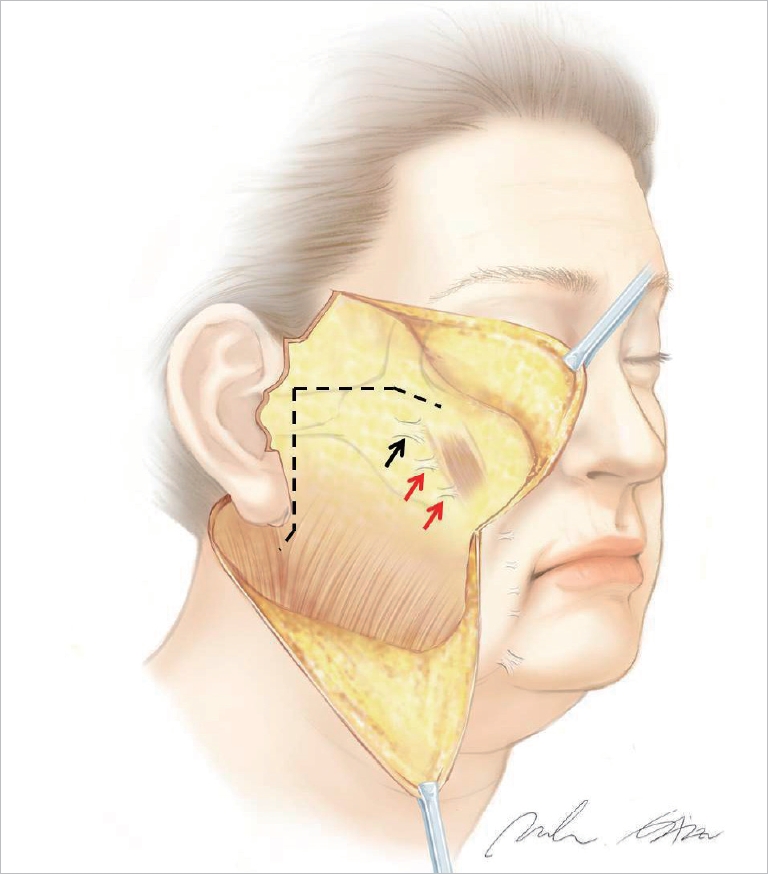
Facelifts using the FAME technique first involved the lifting of the malar fat pad, as its elevation improves the appearance of the midface [17]. The dissection plane for this method is the avascular, soft region underneath the malar fat pad and over the SMAS and muscles [18]. The dissection landmarks of the FAME technique are the inferolateral fibers of the orbicularis oculi muscle and the zygomatic and buccal branches of the facial nerve [18]. After the malar fat pad is mobilized free from surrounding tissues, it is repositioned between the zygomatic body and arch, and fixed to the periosteum [18]. Facelifts using the FAME technique improve mid- and lower facial sagging, elevating the malar fat pad through the prezygomatic space under the orbicularis oculi muscle (Fig. 3) [3]. This method often extends the duration of postoperative edema due to the wide dissection. In midface volume deficiency, fat grafts for volume enhancement may be limited. Malar fat pad elevation without the release of the zygomatic and upper masseteric retaining ligaments may be less effective for midfacial sagging, as Asians tend to have tougher and more rigid retaining ligaments. Therefore, the release of retaining ligaments should be accompanied by malar fat pad elevation to obtain better result in Asians.
High SMAS facelift
A traditional SMAS elevation done about 1 cm below the zygomatic arch cannot correct the midface effectively, because the effect of pulling the flap is limited to the lower cheek regions [5]. To overcome this limitation, the high SMAS facelift was developed, in which the extended dissection of the midface tissues medially and elevation of the flap above the upper border of the zygomatic arch are performed (Fig. 4). This technique influences the midface, infraorbital, and perioral regions, as well as the lower cheek and jowls [5]. The skin and SMAS flap are not separated completely using Dr. BartonŌĆÖs method. The SMAS flap is dissected to the lateral border of the zygomaticus major muscle, and then the flap is dissected in the subcutaneous plane anteriorly from the lateral border of the zygomaticus major muscle. Depending on the depth of the nasolabial fold, subcutaneous dissection can be extended medially [4]. If the dissection is to the nasolabial fold, which is wide in Asians, the risk of bleeding is higher, and because of the zygomatic prominence, it is difficult to visualize. Dr. Marten, on the other hand, preferred a lamellar dissection of the skin and SMAS flap, which allows each flap to be pulled with different amounts of tension and in different directions [5]. SMAS flap elevation is accompanied by a release of the zygomatic and upper masseteric retaining ligaments in the sub-SMAS plane, and it is less wide than Dr. BartonŌĆÖs method. Therefore, the risk of hematoma is lower.
DISCUSSION
There are various retaining ligaments in the face [19]. The zygomatic and upper masseteric retaining ligaments have a direct impact on facelifts, whereas the other ligaments are incidental. The zygomatic ligaments suspend the soft tissue over the zygomatic eminence; without a release of these ligaments, repositioning the malar soft tissue as well as improving the nasolabial fold cannot be achieved. The masseteric ligaments are responsible for supporting the soft tissue of the cheek over the mandible, which must be released to correct sagging of the lower face. Mandibular ligaments are located in the lower anterior portion of face; therefore, these ligaments are not barriers in the superoposterior direction. It is very risky to release these ligaments in the sub-platysmal plane, because it is difficult to secure the surgeonŌĆÖs field of vision, and there are branches of the facial nerve and vessels around the mandibular ligaments. Additionally, maxillary ligaments are located outside the area to be lifted. Thus, these ligaments do not directly affect facelifts [20].
SMAS flaps with release of retaining ligaments in the sub-SMAS plane greatly improve facial sagging. If the retinacular cutis, which is a retaining ligament in the subcutaneous plane, were released in this plane, the skin flap would play an important role in the facelift. In addition, postoperative morbidity, such as scars, ear deformities, and relapse, would be higher, because the skin is not sufficiently tough and rigid to endure a lifting force. Thus, the SMAS flap, which is a tough and rigid tissue, has a main role in facelifts with the proper release of retaining ligaments in the sub-SMAS plane.
Care must be taken when dissection occurs near major structures, such as facial nerves, muscles, and the parotid duct, adjacent to the zygomatic and masseteric ligaments. We use a tumescent solution for hydrodissection to provide a bloodless visual field. In addition, blunt Metzembaum scissors are commonly used for the release of these ligaments without the need for sharp dissection. Since the nerve runs obliquely and the ligaments are oriented vertically, the release should be performed in the upper portion. In this manner, ligaments can be reliably released and injury to the nerve can be avoided. In cases where the ligament and facial nerve branches are difficult to differentiate, then a nerve stimulator may be used to distinguish them.
We believe that the release of retaining ligaments is more important than malar fat pad elevation through the prezygomatic space and SMAS dissection above the upper border of the zygomatic arch for optimal facelift results. If the zygomatic and upper masseteric retaining ligaments are not released in the sub-SMAS plane, other procedures would only secondarily achieve good facelift results, because these ligaments act as barriers in the superoposterior direction.
In most Asian patients, the skin is thicker and more fibrous than that of a typical Caucasian. Asians also tend to have tougher and more rigid retaining ligaments. Facial features are flatter and wider due to prominent zygomas, zygomatic arches, and mandibular angles. Thus, achieving satisfactory results is a challenge [21-23]. The addition of other procedures as well as the release of the retaining ligaments would help maximize facelift effects in Asians. The disadvantage of this method is the relatively long duration of postoperative edema, which is likely due to the need for a wider dissection for better results in Asians. Furthermore, another disadvantage of extended dissection in the sub-SMAS plane is the long learning curve for surgeons to master the technique. Additionally, scarring is a major issue in facelifts, especially in Asians. SMAS flaps should be responsible for lifting, not the skin, which could be closed under no tension to minimize the risk of scarring. It is also very important that the retaining ligaments are dissected in the sub-SMAS plane, as the SMAS flap greatly affects facelift outcome.
CONCLUSIONS
Achieving satisfactory facelift results is relatively difficult in Asians. The release of retaining ligaments in the sub-SMAS plane is the most important step during Asian facelifts for satisfactory results. The addition of SMAS dissection above the upper border of the zygomatic arch and malar fat pad elevation through the prezygomatic space help achieve better results for Asian facelifts. More studies are necessary to redefine suitable facelift methods for Asians.