INTRODUCTION
Synmastia is serious condition but rare and defines as any situation in which the breast implant crosses the midline, even if it is only on one side. Synmastia is a technical complication caused by over-dissection of the medial pocket over the sternum. Use of large breast implants with a significantly larger than the base of the breast can contribute to synmastia formation [1,2]. In Korea, as the volume preference of doctors and patients tends to be larger recently, the possibility of medial over-dissection is also increased.
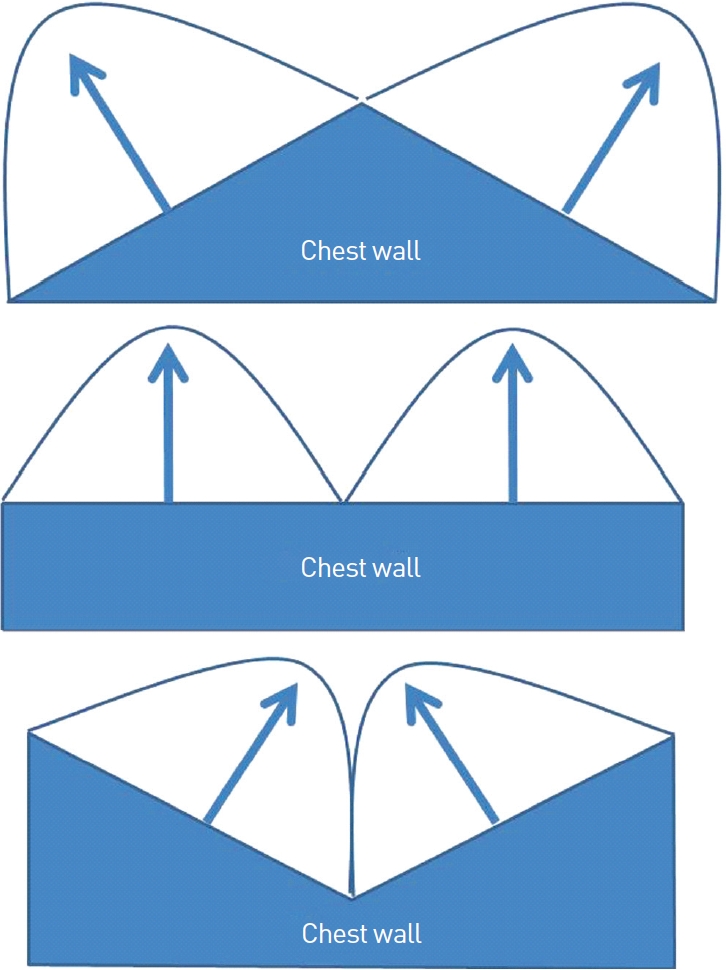
Implants push overlying soft tissue in the direction of the right angle from the chest wall (Fig. 1). In most cases, chest wall contour is convex and directs slightly outward, so the divergence of the breasts and wide intermammary distance is more frequent complaint of the patients who expect narrow valley between breasts (Fig. 2A). However in the patients of sunken chest, the possibility of synmastia increases in breast augmentation of sunken chest. So surgeons should be careful not to make the pocket too medially for the prevention of synmastia. Even after making the pocket as wide intermammary distance, there are continuing forces to push implant medially, such as muscle action, slant and the elasticity of laterally elevated soft tissue (Fig. 2B, C).
As Pectoralis major muscle contracts, the implant tends to move in medial direction and to act as a wedge in sunken chest. The attached origin of Pectoralis major muscle is gradually detached and synmastia may occur (Fig. 3). This tendency in sunken chest is more apparent with smooth shell implants. Aggressive overdissection of medial portion is the exact cause of synmastia, however similarly limited dissection at the sternal area may be safe or vulnerable to synmastia according to the convexity or concavity of chest wall.
Case 1 is the patient who visited my clinic for the correction of synmastia. She got breast augmentation with smooth shell saline implants 1 year before visiting my clinic. Right implant displaces medially and crosses midline. After removal of implant, sunken chest is shown. Costal angle of right anterior axillary line is very acute and less than 90 degree. This sunken chest is not direct cause but one of predisposing factors of synmastia (Fig. 4).
I have an idea from buttock augmentation with implant. For buttock augmentation, implants place intramuscularly for the protection of sciatic nerve and for the prevention of implant displacement [3]. Muscle splitting concept for intramuscular placing of implant in sunken chest adds tissue to sunken area and provide guarding barrier to reduce detaching tendency at the parasternal area.
METHODS
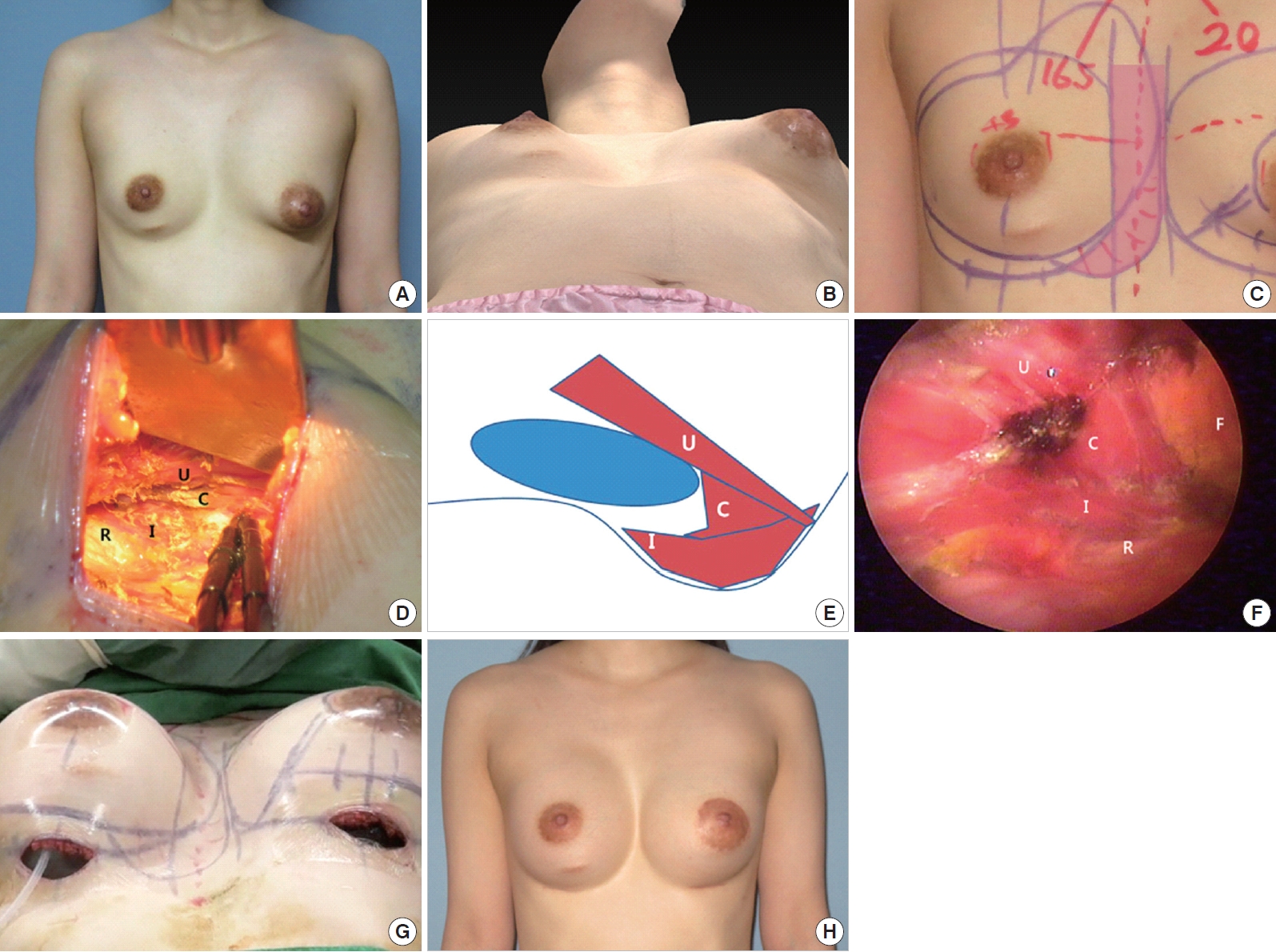
Case 2 is 28 years old nulliparous woman. She has severe asymmetric chest wall and breasts; sunken right chest wall and sternum which is more severe in lower half of the chest, left upper ribs protrusion, left tuberous breast, different position and size of nipple areolar complex, and different shape and size of both breast. During planning operation, my concern is not to make the perfect result, but to prevent disaster. For similar size after operation I have to quite larger implant for left breast. sunken chest with large implant is regarded as the receipt of synmastia. So I considered intramuscular placing implant at lower medial corner of the subpectoral pocket which means not to elevate lower medial origin of Pectoralis major from the costal cartilage but to split the muscle partially with remaining the muscle to the bed. These multiplane, irregularly directed muscle stripe resist to detaching force. En bloc elevation of lower medial pectoralis major muscle makes larger submuscular space and easily extended more medially. Irregular muscle splitting of medial sunken area reduces slope degree and more resist against detaching force as intramuscular buttock augmentation. This concept of intramuscular placement acts as a guarding effect from medial displacement (Fig. 5).
RESULTS
After I had the concept of intramuscular placement for the breast augmentation in case of sunken chest, I experienced steady medial breast contour in 5 sunken chest cases with the same concept. Although 4 months follow-up photo of case 2 is not enough to estimate medial displacement tendency of implant, medial breast contour is well maintained.
DISCUSSION
Spear (2006) reported some characteristics of postaugmentation synmastia All of the implants were subpectoral. The majority of these women had undergone more than one operation. Many of them had undergone successive operations to enlarge the size of their implants and breasts. Many of them had large implants, arbitrarily defined by us as greater than 400 cc or with a diameter of 14 cm or more. Several of the patients had associated chest wall skeletal deformities, and some had undergone simultaneous mastopexy at the time of their breast enlargement.
For the synmastia, prevention is better than a successful repair. Nowadays many women want large implant. For the patient of sunken chest, smaller implant is better, and more restricted medial dissection is required for the prevention of synmastia.
Spear (2004) named unilateral sunken chest as anterior thoracic hypoplasia which shows hypoplasia of the ipsilateral breast, superior location of the nipple-areola complex compared with the contralateral side, and normal Pectoralis muscles. This paper shows that implants of affected sites displaced more medially.
For buttock augmentation implant is placed intramuscularly in Gluteus maximus muscle for the protection of sciatic nerve and the prevention of implant displacement. This concept is effective for the medial displacement of implant in breast augmentation of sunken chest. This concept of intramuscular placement of implant is also applicable for reducing lateral displacement in case of pigeon chest. In this case, muscle splitting is done at the lateral portion of pectoral muscle.
CONCLUSION
For the patient of sunken chest, smaller implant is better, and more restricted medial dissection is required for the prevention of synmastia. Muscle splitting as coronal plane of medial portion of pectoral muscle make muscular pouch at the medial corner of subpectoral pocket which is effective for the prevention of medial displacement of implant in breast augmentation of sunken chest by guarding effect of irregularly arranged muscle fibers which resist against the detaching force of pectoral muscle from the sternocostal origin.