Reconstruction of Defects after Removal of a Kissing Nevus of Eyelids using a Tissue Expander
Article information
Abstract
The kissing nevus is a rare form of congenital melanocytic nevus. We present a case of a 4-year-girl with kissing nevus on the right eyelids. As a treatment, we used a tissue expander. In the first operation, The 16 cc sized rectangular-shape tissue expander was inserted within the subcutaneous layer at the right zygomatic area. After expansion for 5 months, local advancement flap was performed for lower eyelid reconstruction, and interpolation flap was carried for the upper eyelid. The remnant interpolation flap was removed and trimmed after 3 weeks. We report here a rare case of the kissing nevus on the eyelids that showed good results after reconstruction using a tissue expander.
I. INTRODUCTION
The kissing nevus (or divided nevus) is a rare congenital pigmented lesion, which are located in the adjacent area [1]. Because the nevusinvolves both the upper and lower eyelid margins, the edges of the eyelids are in contact during blinking. For this reason, we call it the kissing nevus. The nevus arises from the melanoblasts or Schwann cells of the neuroectoderm. The eyelids begin to form at 5~6 weeks of gestation and fuse at 8~9 weeks of gestation. Then, the eyelids separate at 24 weeks of gestation. Therefore, the kissing nevus of the eyelids formed when the nevus originated at 8~24 weeks of gestation and melanocyte moved to another side of the eyelid [2,7-9]. It was first reported by Von Micheal in 1908 and named for the first time by Fuchs in 1919 [1]. The most frequently reported kissing nevus is the one of the eyelids. In addition, there are a few reported cases of the fingers and the penis [3,4].
The authors report the reconstruction using a tissue expanderin a patient with kissing nevus of the eyelids.
II. CASE
A 4-year-old girl was admitted to our hospital for congenital kissing nevus on the right upper and lower eyelids. The nevus was round in shape and 3 × 3 cm in total size. The nevus occupied about half the full width of the upper eyelid and accounted for about 70% of the entire width of the lower eyelid (Fig. 1). It did notrise and cause pain.

Preoperative photograph. Kissing nevus was on right upper and lower eyelids and was 3 × 3 cm in total size. Photograph taken during blinking (A) and closing (B).
At the first surgery, the incision was made along the bottom edge of the right lower eyelid and was extended to the lateral canthal area. After subcutaneous dissection to the right zygomatic area, the authors put a 16 cc, 4 × 2 cm sized rectangularshape tissue expander (Fig. 2). We did not inject normal saline at this time.

Photograph taken before a tissue expander insertion. Using the incision line, we dissected for pocket formation at the subcutaneous layer. The tissue expander (rectangular 16 cc, 4 × 2 cm size) and port were inserted. Initial inflation was not carried. OR, orbital rim.
From 26 days after the first surgery to 5months, normal saline of 2.5 cc to 4 cc was injected to the tissue expander every week over 12 timesin total of 33.5 cc. Then, the tissue expander wasremoved and the nevus was excised. The authors preserved the grey line of the eyelids. The nevus was located within the deep dermis. We made a triangular transposition flap for the back-cut, which is made for the rotation of the expanded flap to reconstruct the defects after nevus excision (Fig. 3). We temporarily checked whether we could reconstruct the defects. We divided the expanded flaps to reconstruct both defects on the upper and lower eyelids. Local transposed flap was performed forthe lower eyelid reconstruction. The upper one was made as an interpolation flap because the nevus was apart from the expanded flap.The canthotomy, cantholysis and tarsoconjunctival lamina surgery was unnecessary. The flap was not anchored on the periosteum because the skin expansion was enough for us to redrap the flaps without tension. The sagging and the pouting of the lid margin did not occur.
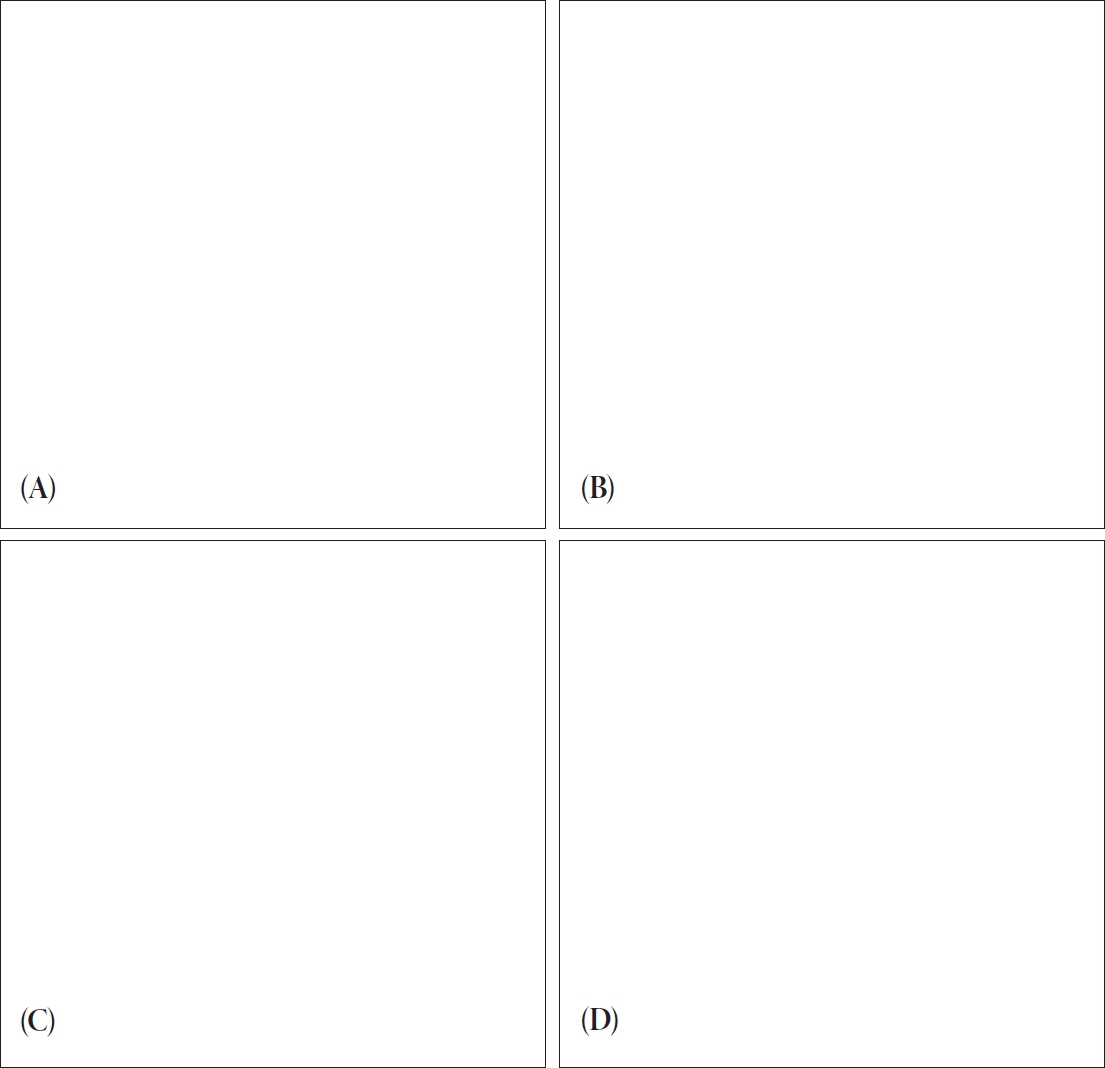
Photograph taken at 2nd operation. (A) Operation design. We made a triangular transposition flap (★) for the back-cut which is made for the rotation of the expanded flap to reconstruct defects after nevus excision. (B) Nevus excision and the tissue expander removal. (C) We temporarily checked whether we could reconstruct the defects. We divided the expanded flaps to reconstruct the both defects at upper and lower eyelids. The upper one was made as an interpolation flap because the nevus was apart from the expanded flap. (D) Final postoperative photograph. Look at the transposition flap for the lower eyelid and interpolation flap for the upper eyelid.
The remnant interpolation flap was removed and trimmed after 3 weeks (Fig. 4). These showed good results without complications, such as scar contracture and ectropion until 5 months after the last surgery. There was no significant difference in the skin texture (Fig. 5).

Photograph taken after the removal operation of remnant interpolation flap.
Photograph taken 5 months after the last operation. These showed good results after reconstructing using the tissue expander.
III. DISCUSSION
Congenital nevus appeared in about 1% of live births. They varied in size, but most of them were less than 1.5 cm [5]. We do not know the exact incidence of malignant transformation about small nevus. Nevus that were larger than 4 cm tended to have approximately 4.6% risk of malignant transformation in 30 years [6]. The kissing nevus on the eyelids could cause problems, such as poor aesthetics, ptosis, visual field defects and epiphora. It is important to completely remove the nevus at the time, otherwise, it could regrow and become wart-like or thick. In addition, the risk of malignant transformation could increase and the reconstruction after excision might be difficult.
The upper eyelid ptosis, visual field defect and deprivation amblyopia could occur in patients with kissing nevus on the eyelids. The symptom might occur especially in the early childhood or adolescence. The disfigurement got worse over time and there was a possibility of malignant transformation. Therefore,surgeons mustremove kissing nevus at an early age [10].
Various methods have been introduced for the reconstruction after the removal of kissing nevus on the eyelids. However, surgical protocol of kissing nevus has not exactly been established. It is not easy to reconstruct two area of symmetrical position at the same time. The surgeons should apply appropriate methods depending on the size and location of nevus. In general, early reconstruction showed good cosmetic results. The dermabrasion had a possibility of high recurrence because the nevus cells in the deep dermis could survive. If nevus occupies about 25% of width of the eyelid, it is possible to reconstruct with primary closure. In cases of larger nevus, we could use local flap, such as semicircular flap [11]. The lateral canthal, semicircular flap might be used for reconstruction of a central eyelid defect [12] The basic method of reconstruction included the semicircular flap, lateral canthotomy, inferior cantholysis and triangular excision. The skin and muscle incision began at the ateral canthus in a semicircular fashion. A lateral canthotomy was performed beneath the flap and inferior portion of the lateral tendon was cut. A triangular area beneath the defect must be excised for preventing dog-ear deformity [12]. Besides, we could use the tarso-conjunctival flap with skin graft and musculo-cutaneous flap. In large kissing nevus, the surgeons could take full-thickness skin graft from post-auricular area or contralateral eyelid [13]. However, skin graft could produce unsatisfactory results because the color and texture of the skin does not match each other. The several rounds of surgery might be necessary in large kissing nevus. Staged excision, at intervals of 6 months or 1 year, might be needed many times and had the high possibility of scar contracture.
The tissue expander surgery was a simple and established reconstructive method. The advantage of this method is that we could use the same color and texture of the skin, as well as soft tissues. Nevertheless, the skin around the eyes is soft, weak and does not have hair. For these reasons, most frequently performed eyelid reconstruction using the tissue expander was skin grafting after expansion of the supraclavicular area. However, the authors expanded the zygomatic area,right next to the eyelids, and reconstructed both the upper and lower eyelids by local flap at a time. It was difficult to reconstruct two areas of symmetrical position at the same time, it was especially more difficult to reconstruct the upper eyelid. The local flap or skin graft for the upper eyelid surgery was required. This procedure had high risk of the ectropion. We used the interpolation flap for the upper eyelid reconstruction. The remnant interpolation flap was removed and trimmed later. These showed the good resultswithout any complication.
The authors could confirm that reconstruction using the tissue expander showed good results in a rare case of kissing nevus on the eyelids.
Acknowledgements
This work was supported by the Seoul National University Brain Fusion Program Research Grant.