Concept of Reduction Malarplasty
Article information
Abstract
Reduction malarplasty is one of the most frequently performed facial contouring surgeries in eastern Asia. Intraoral approach makes the most of the part, and coronal approach is used in revision cases or older patients who consider simultaneous lifting. In most reduction malarplasty cases malar highlight area is moved medially or posteriorly. The ostectomy should focus on medialization of the body, not reducing the volume. It is better to perform fixation on both body and arch of malar bone. Fixation of the body should at least be done with separate two bridges across the ostectomy line. Risk factors of sagging include low skin elasticity, abundant soft tissue, old age and deep nasolabial fold. The patients with these factors should be explained thoroughly about postoperative cheek drooping. Accurate planning of reposition and solid fixation should always be done.

Reduction malarplasty is one of the most frequently performed facial contouring surgeries in eastern Asia. Recently, as the number of three-dimensional computed tomography is growing, patients’ demand gets fastidious about postoperative feature, and more concerns appeared to various surgical complications. Complications such as inferiorly displaced nonunion of malar complex, bony gap of malar body area and soft tissue drooping are frequently discussed problems with cosmetic dissatisfaction [1-3]. Therefore, in this article I would like to discuss about surgical approach, reposition and fixation, and prevention of cheek drooping.
I. APPROACH
Two main approaches in reduction malarplasty are coronal and intraoral [4-6]. There are several pros and cons in both approaches, but intraoral approach makes the most of the part, because patients in these days mostly demand smaller incisions and shorter downtime, and also especially Asian patients tend to avoid coronal approach.
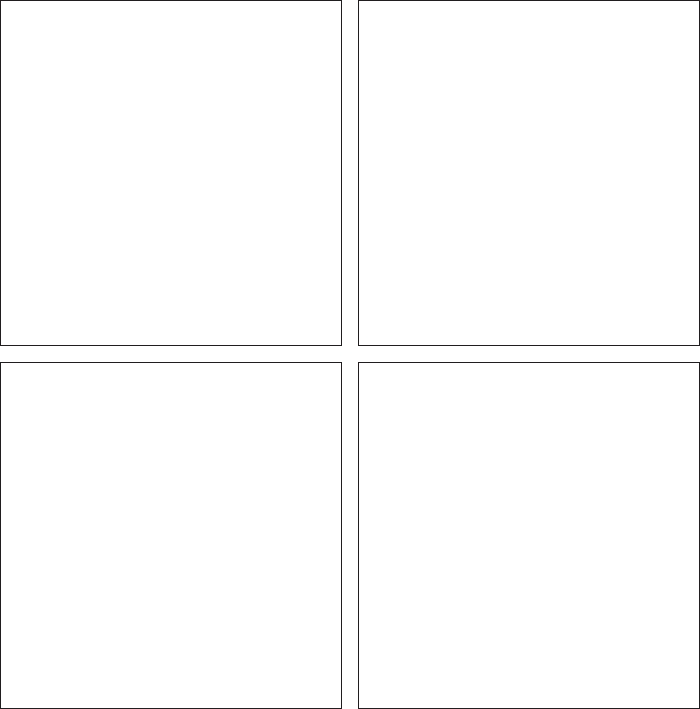
Because coronal approach allows better view of whole malar complex, more accurate reposition is possible. Also, as it is possible to make fixation on the upper part of the malar body, more stable fixation is possible against rotation force of masseter. On the other side, surgical time is quite longer, and the possibility of frontal branch injury or temporal area depression exists [7,8]. Therefore, coronal approach is used in revision cases or older patients who consider simultaneous lifting. To overcome the difficulties of malar complex approach by previous intraoral approach of sideburn incision, and to obtain calvarian bone as a bone graft donor in cases with bony gap, coronal approach should be performed (Fig. 1).
Revision reduction malarplasty was done via coronal approach. The intraoperative photograph shows malar body fixation.
To minimize temporal depression, damage of malar fat pad should be avoided by performing dissection between temporoparietal fascia and superficial layer of temporalis fascia [7]. The possibility of traction injury of frontal branch should be informed and receive consent from the patients before surgery, although usually it is temporary and improves in several months. Also, because patients tend to suffer cheek drooping from previous surgery, simultaneous midface lift should be always considered [1].
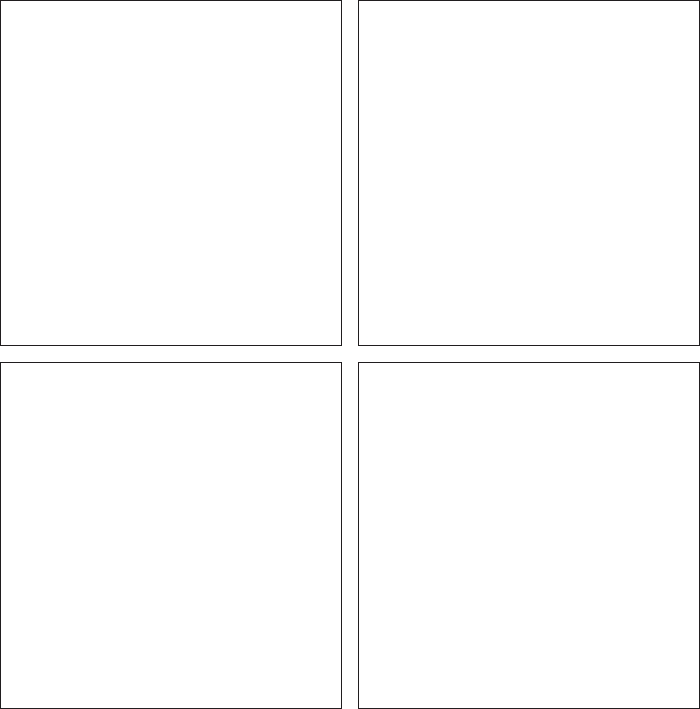
Intraoral approach is mostly used in primary cases, for its shorter operation time and less downtime. With intraoral incision to approach malar body, preauricular or sideburn incision is usually added to reach malar arch (Fig. 2) [9,10]. Occasionally arch osteotomy is performed via intraoral approach or temporal incision inside the hairline, but in these cases fixation of arch is impossible. With intraoral approach, buccal fat pad can be removed and skeletal augmentation of paranasal or anterior cheek area with implant can be performed at the same time. Also same incision can be used when performing with two jaw surgery. But extra caution should be given to accurate osteotomy, reposition and fixation, as numerous complications can be possible such as bony gap of malar body, inferior displacement of malar complex, and outward protrusion of arch area from inappropriate arch fixation [11].
Malar body reposition and fixation via intraoral approach.
II. REPOSITION
‘Reduction’ in reduction malarplasty does not actually mean reduction in size of the bone, but rather stand for minimizing protruding looks of the most prominent part of the malar body [12]. Similar concept is found in prognathism cases, which the surgeon makes the chin look smaller by rotating the bone by setback operation. Therefore, ‘reposition’ malarplasty makes more sense and can be a more correct term than reduction malarplasty.
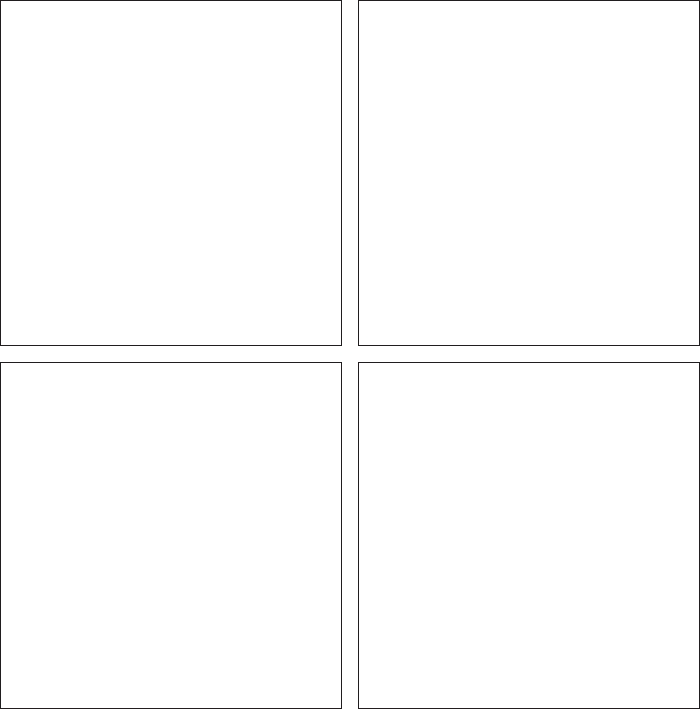
Malar bone is relatively small. Analogous to prognathism cases, the location of the bone, not the size, is responsible for protruding appearance of the malar bone. Therefore, performing excessive rasping or ostectomy in order to reduce the bony volume can result in insufficient postoperative outcome and complications such as soft tissue problems and bony malalignment (Fig. 3) [13].
Bone defect occurred from excessive rasping of malar body (Left) and arch (Right).
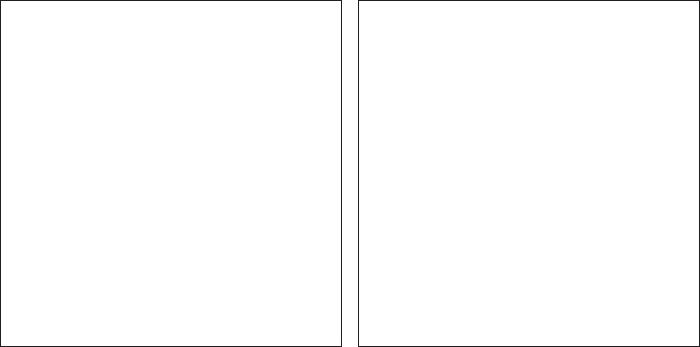
Malar complex can be divided into malar body and arch, which the patients designate as ‘45-degree malar’ and ‘side malar’, respectively. If arch is prominent, bony Z-plasty is performed, as outer cortex of malar complex and posterior portion of arch attached to the skull makes bony contact (Fig. 4, 5) [5]. As the ostectomy line moves posteriorly toward the skull, the amount of internal rotation of the arch gets bigger. But excessively posterior ostectomy line can prevent arch rotation and makes the fixation difficult. Also, excessive internal rotation of the arch can cause soft tissue depression, and ‘boxy’ frontal appearance when it is not harmonized well with malar body ostectomy.
(Left) The face looks broad by overdeveloped arch. (Right) As arch area gets narrow by reduction malarplasty, the patient can have more slender looking face.
(Left) In first operation, arch was left unchanged when malar body was effectively reduced. (Right) Reoperation was done to reduce the arch.
Body prominence mainly relies on the location. Malar highlight, the most prominent part of the malar bone, has most protruding looks when it is located externally, anteriorly and superiorly, and vice versa. Balanced location of malar highlight allows healthy, younger looking face, as too much protrusion gives masculine, bumpy facial shape, and too weak highlight resultsin cheerless, olderimpression (Fig. 6) [14].
Although reposition of arch has limitations because of wide skull, the face looks smoother as malar body prominence is reduced. (Left) Preoperative photographs. (Right) Postoperative photographs.
Therefore, in most reduction malarplasty cases malar highlight area is moved medially or posteriorly, as inferior movement can cause soft tissue sagging (Fig. 7). Ostectomy of the medial portion of the body is needed in medial reposition. The ostectomy should focus on medialization of the body, not reducing the volume [15]. The amount of the ostectomy is not related to decreasing malar body prominence, and excessive amount rather cause difficulties in bone to bone contact after malar body reposition. The most frequent location of contact loss is upper area around the orbital rim, because the area can be most vulnerable from pulling action of the masseter as the fixation is usually performed at the lower part [3]. Large gap can be palpated and lead to depression, and sensitive patients can have complaints although the gap itself does not induce functional problems (Fig. 8) [11]. The gap between the ostectomy lines should be smaller in the upper portion, and performing the ostectomy in perpendicularfashion can avoid the bony gap.
(Left) In first operation, malar body was left unchanged while arch was successfully reduced. (Right) Reoperation was done as malar body was repositioned medially and posteriorly.
(Left) Excessive bone resection of malar body produced bone defect without reducing malar body prominence). (Right) Bone gap can grow bigger when one-point fixation is done near the orbital rim.
Setback of the malar body is another option of reducing malar prominence without concerns of making bone gap like in medialization. But the surgeon should always consider soft tissue changes, as excessive medialization or setback of malar body can result in soft tissue drooping, like in two jaw surgery when too much maxilla setback lead to upperlip drooping. Occasionally, to minimize soft tissue sagging, superior or anterior movement and fixation of the malar complex is performed after ostectomy, but the surgeon should be cautious about increased body prominence.
III. FIXATION
Fixation is the key element of the reduction malarplasty. There are cases which fixation is both performed at body and arch, body or arch alone, and cases without any fixation [16-18]. Wires or plates and screws are used, and recently absorbable plates and screws are also being used [6,19].
It is better to perform fixation on both body and arch of malar bone, as two-point fixation reassure accurate reposition. But fixation alone cannot control all the problems, such as inferior displacement or bone gap on superior portion when operation is done under concept of reduction, not reposition and when too much bone is resected or only one-point fixation is performed [2]. Therefore, fixation should at least be done with separate two bridges acrossthe ostectomy line [1]. If fiation is not done on the arch area, ticking sound can be heard before complete bony reunion on mastication and the surgeon should receive consent before surgery. Arch can be repositioned externally after the surgery when fixation is not done, so if possible, arch fixation is recommended.
If the surgery only localized to arch area and no reposition of malar body is needed, no fixation can be done without any complications. But such cases are small in proportion, and patient selection of this method should be made with caution. Of course,rigid fixation must be done if body reposition is considered (Fig. 9).
Fixation must be done when reposition of the body is considered. If not, lateral and inferior displacement can be occurred by masseter action.
IV. CHEEK DROOPING
The most wondered and feared consequence of reduction malarplasty would be postoperative soft tissue sagging. The amount of soft tissue sagging does not always goes with the amount of bone reduction, as the arch area, the part with most reduction, consists of not much soft tissue nor lead to sagging. The area which sagging most frequently occur is malar body area, and thus surgeons should pay more attention to soft tissue sagging when performing body reposition [11].
The main causes of cheek drooping can be consisted of dissection area, soft tissue remained to the body, drooping of the bone, and change of malar body prominence. Although large dissection area can lead to more injury to retaining ligaments that support the soft tissue, the dissection itself is not thought to be the main factor. Rather, operating without accurate exposure can make more problems. Usually, soft tissue is tightly anchored at more medial and lateral portion of the malar body than ostectomy line, and excessive dissection at these areas are not needed.
Risk factors of sagging include low skin elasticity, abundant soft tissue, old age and deep nasolabial fold. The patients with these factors should be explained thoroughly about postoperative cheek drooping. Simultaneous midface lift, buccal fat removal, and paranasal augmentation can be helpful in reducing the risk (Fig. 10).
Abundant soft tissue of malar body and low skin elasticity preoperatively (Left) can lead to deeper nasolabial fold by redundant soft tissue postoperatively (Right).
In cases ofsoft tissue drooping from inferiorly displaced malar bone caused by inappropriate reposition or fixation, reoperation should be considered. When bony gap is narrow or approach by existing incision is possible, intraoral approach can be used again. But if the gap is too wide and bone graft is needed and approach is difficult, coronal incision should be considered (Fig. 11) [1].
(Left) Cheek drooping caused by inferior displacement of bone from nonunion. (Right) Bone graft after reposition via coronal approach can be helpful.
The change of malar body prominence can be mistaken as cheek drooping. Weaker malar body prominence can lead to tired, elderly appearance and some patients complain about cheek drooping, in spite of no soft tissue sagging [14]. As this condition is difficult from actual sagging, the patients should receive information before the surgery. And the surgeon should always consider soft tissue change and appearance when planning malar prominence reposition (Fig. 12).

(Left) A preoperative photograph and a 3D CT. (Right) Tired and elderly looking impression can be found postoperatively without any skeletal problem. Weaker malar highlight can be a cause, which is frequently confused with cheek drooping.
V. CONCLUSION
In conclusion, reduction malarplasty is a surgery that change the shape and location of malar bone not by bone reduction, but by reposition of malar complex to more aesthetic location and thus make more slender, soft appearance. Thus, besides reduction of the bone, accurate planning of reposition and solid fixation should always be done. Also, consideration of soft tissue is essential, and careful patient selection and through preoperative consultation isimportant.