지방흡입물로부터 추출한 기질혈관분획의 분석
Analysis of Stromal Vascular Fraction from Lipoaspirates: Our Institute's Experiences.
Article information
Trans Abstract
Today, adipose tissue derived mesenchymal stem cells (ADSC) have gained a great interest in various medical fields due to the characteristics of its self-renewal and multilineage differentiation capacity. The stromal vascular fraction (SVF) of adipose tissue is known to contain mesenchymal stem cells and it is obtained by processing the lipoaspirate which is usually collected from tumescent liposuction. In this study, we reviewed the records of patient epidemiology and results of SVF isolation. 30 patients (8 males and 22 females) had been underwent tumescent liposuction between April 2012 and January 2013, and the collected lipoaspirates were processed to isolate SVF in GMP facility in CHA Bundang Medical Center. The average stem cell count per 1 cc of lipoaspirate was 52,252 ± 26,704 and cell count including red blood cells per 1cc of lipoaspirate was 970,607 ± 873,436. The stem cell viability was proven to be 84 ± 4%. Bacteria were not detected in all the SVF samples. Compared to previous reports concerning the yield of SVF, our results coincide well with the results of previous studies. Because there were no domestic report about the yield and viability of SVF, this report may provide a reference value of the Korean SVF for the clinicians who want to use SVF as a therapeutic purpose.

I. INTRODUCTION
In recent years, adipose tissue derived mesenchymal stem cells (ADSC) have gained a great interest in plastic and reconstructive surgery. ADSC have strong paracrine effects and can be differentiated into various types of cells, such as osteoblasts, chondrocytes, endothelial cells, myoblasts, and adipocyte [1]. Studies have revealed that ADSC have the ability to promote wound healing process, accelerate angiogenesis in ischemic conditions and secrete anti-inflammatory cytokines [2]. But practically, stromal vascular fraction (SVF) rather than ADSC is used because pure ADSC can be obtained by multiple times of culture and there were some legal issues in clinical application of ADSC to patients.
Human adipose tissue is available in large quantities and is easily collected via relatively simple surgical procedures. The two most commonly used methods are surgical resection of fat tissue and liposuction, which are different types of body contouring plastic surgery procedures. Thanks to the minimal patient discomfort and little donorsite morbidity, liposuction is believed to be the best way for adipose tissue harvesting [3].
A good manufacturing practice (GMP) facility is a produc tion facility or a clinical trial materials pilot plant for the manufacture of pharmaceutical products. It includesthe manufacturing space, the storage warehouse for raw and finished product, and support lab areas for medical grade uses. Our institute established GMP grade facilities for SVF isolation about 1 year ago. In thisstudy, we reviewed the records of patient epidemiology and results of SVF isolation from our GMP facility (GMP facility in CHA Bundang Medical Center).
II. METHODS
A. Tumescent liposuction
Human subcutaneous adipose tissue samples were collected from the patients who were scheduled to undergo cosmetic fat graft, body contouring and orthopedic clinical trials. Tumescent technique was used to obtain adipose tissue from the abdomen, flank and thigh. In detail, a hollow blunt-tipped cannula was introduced into the subcutaneous space of the donor site through a small stab incision. A 1000mL of 0.9% NaCl saline solution, supplemented with 1 mg of epinephrine and 400mg of lidocaine was manufactured and infiltrated into the adipose compartment to minimize blood loss, pain and tissue contamination by peripheral blood cells prior to liposuction. Fifteen minutes after injection, subcutaneous adipose tissue was aspirated with gentle manual suction.
B. Isolation of ADSC
The collected lipoaspirate was immediately transported to laboratory in sterile manners and centrifuged at 400g for 5 minutes. After removing tumescent solution in the lipoaspirate, the volume of adipose tissue is measured and this value is considered as the initial volume of adipose tissue obtained by liposuction. Prior to beginning the procedures, each enzyme mixtures and buffer (Phosphate buffered saline + 2% gentamicin) were warmed up in the 37℃ water bath.The adipose tissue was washed with an equal volume of warm buffer, followed by centrifuging at 400g for 5 minutes at room temperature. After carefully removing the top layer of oil, disposable pipette (2ml or 5ml) was used in aspirating the floating adipose tissues. Then, the adipose tissue was mixed with an equal volume of enzyme mixture, containing trypsin (Sigma-Aldrich, St. Louis, USA), dispase (Life technologies, Carlsbad, USA) and collagenase I (Life technologies, Carlsbad, USA), reacted at 7g for 60 minutes in the 37℃ shaking water bath for tissue digestion. To block the enzyme effect, about 10cc of patient’s blood was centrifuged at 1120g for 5 minutes at room temperature, and the upper layer of plasma was separated in one 50 mL conical tube. Then, the plasma was added to the solution and set plasma’s volume to 5% of the whole volume ofsolutions. Quality control sample was collected after a couple of saline washing, centrifuging and separating procedures. 10ul of solution was taken to mix with 10ul of trypan blue dye. And then, we counted the number ofstem cells using with a hemocytometer. Cell viability was assessed using the trypan blue dye, discriminating the colors of the cells. Cellsurface markers, such as CD44, CD73 and CD105 were set as positive markers, but simultaneously, CD31, CD45 were set as negative markers. Bacteriological examination was performed by the quality control team, part of the GMP facility, with culturing SVF for 14 days.
III. RESULTS
Thirty patients (8 males and 22 females) had been underwent adipose tissue aspiration between April 2012 and January 2013 by a single surgeon.The median age of the patientswas 56 years, ranging from 19 years to 69 years, and the average body mass index (BMI) was 24.4±2.4, distributed between 18.8 and 30.1. In the majority of patients (90 percent), adipose tissue was harvested from the abdomen, but four patients were determined to collect adipose tissue from the posterior, lateral thigh or buttock. Initial volume of tumescent infiltration before liposuction was ranged from 200cc to 550cc. The average volume of total adipose tissue aspirate was 53.2±26.4cc, ranging from 10cc to 130cc. Total stem cell counts were ranged from 2.5×105 to 7.9×106 , which showed large distribution depending on the total amount of adipose tissue aspirate. Similarly, total stem cell counts including red blood cells (RBC) were distributed between 6.2×106 and 1.9×108 . The trypan blue assay was used to determine stem cell viability, and revealed that 84±4% of the cells, on average, were assessed to be alive. The average stem cell count per 1cc of adipose tissue aspirate was 52,252±26,704, ranging from 10,560 to 110,000. Cell count including RBC per 1cc of adipose tissue aspirate was 970,607±873,436, ranging from 160,000 to 3,960,000. ADSC expressed CD44, CD73 and CD105 (positive cell markers), but CD31, CD45 were not expressed (negative cell markers) (Fig. 1). Quantification of stem cell markersisshown in Fig. 2. Through 14 days of bacteriological examination, bacteria were not detected in all the samples. Patient characteristics and laboratory data are listed in table I.
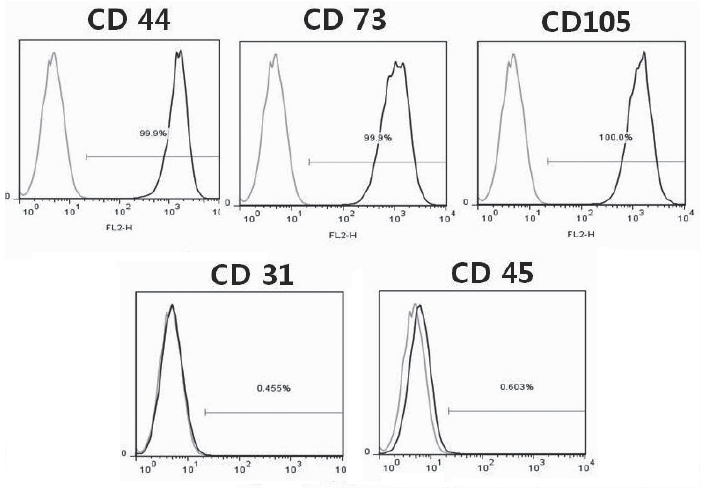
ADSC expressed CD44, CD73 and CD105, but CD31, CD45 were not expressed. ADSC, adipose tissue derived mesenchymal stem cells.
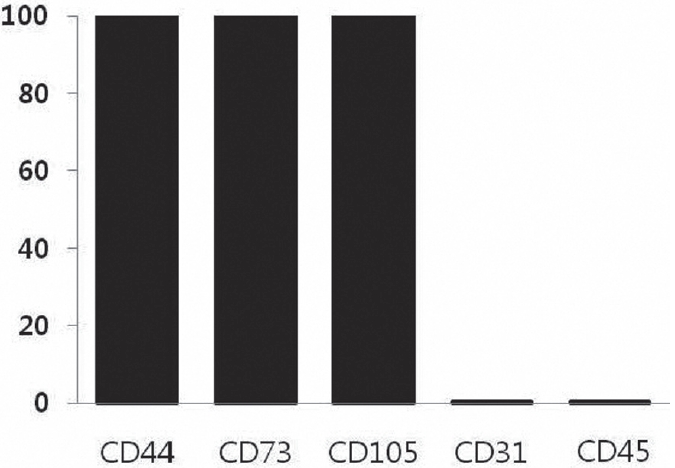
Percent expression of stem cell markers obtained by quantification of immunofluorescent markers in SVF. SVF, stromal vascular fraction
IV. DISCUSSION
ADSC have recently been tested in various types of experimental models for the treatment of human diseases [1,4]. In most of these studies, ADSC were collected from tumescent liposuction techniques. In thisreport, we analyzed ourtwenty-five cas es of tumescent liposuction procedures, which were performed by a single surgeon. The yield and viability of SVF processed by the GMP facility in CHA Bundang Medical Center were presented. In this series of liposuction, no complications were noted and all the patients readily returned to daily life. Adipose tissue harvesting from the abdomen, thigh or buttock is easy and convenient and causes minimal cosmetic problems on donorsite.The collected lipoaspirate wasimmediately transported to laboratory in closed 50 cc syringe because there was a report mentioning that the time between tissue sampling and tissue preparation should be minimized [5].
Although aspirated fat volume was usually more than 100cc per one patient, this lipoaspirate often contained some amount of tumescent solution, RBC and cell debris. Therefore, the aspirate should be centrifuged at 400g for 5 minutes immediately after transferring to the laboratory. After completely removing the remnant tumescent solution, on average, 53.2±26.4cc of adipose tissue was used in producing SVF. The number of viable stem cells isolated from the adipose tissue aspirate was approximately 52,252±26,704 cells per 1mL of lipoaspirate (970,607±873,436 including RBC), and the cell viability tests showed that approximately 84±4% of the ADSC were alive. According to the previous report, processing 1mL of lipoaspirate yielded 4.0×105 ±2.1×105 cells (including RBC) with 93.9±3.3% cell viability. 6 Oedayrajsingh-Varma et al. reported approximately 3.5×104 ±0.1×106 cells per gram of fat tissue and 81±2% viability. 3 Locke et al. reported 2.4×104 cells per 1mL of fat processed, and Muscari et al. showed 3.3×105 ±0.3×105 cells(including RBC) per 1mL of fat tissue [7,8]. Compared to this, it is evident that the yield of SVF manufactured by the GMP facility in CHA Bundang Medical Center coincides well with the results of previous studies.
Use of SVF from lipoaspirates are becoming more popular not only in plastic surgery but also in other medical fields including orthopedic surgery, neurology and etc. The SVF used in these surgical procedures is usually extracted by some kind of commercial machines. However, so far, no domestic reference has been reported yet to estimate the yield and viability of the SVF manufactured by those stem cell extracting machines. The purpose of this study is to provide one reference for the SVF, manufactured with the operation of sophisticated laboratory equipments. We think our data can be a reference for the clinicians who want to use SVF as a therapeutic purpose. Further study will be focused on the analysis of patient’s individual conditions, such as age, BMI, medical history, and amount of initial tumescent,which can affect the yield and viability of SVF.

Patient Characteristics and Laboratory Data
V. CONCLUSION
In this study, we reviewed the records of patient epidemiology and results of SVF isolation. The average stem cell count per 1cc of lipoaspirate was 52,252±26,704 and cell count including red blood cells per 1cc of lipoaspirate was 970,607±873,436. The stem cell viability was proven to be 84±4%. These data can be a reference for using SVF as research or clinical purpose.