Restoration of an Upper Lip Affected by Necrotizing Ulcerative Stomatitis Using Bilateral Cheek Advancement with a Crescentic Perialar Excision
Article information
Abstract
Necrotizing ulcerative stomatitis (NUS) refers to ulceration of the oral mucosa that precedes rapid orofacial soft- and hard-tissue destruction. NUS on the upper lip is considered a reconstructive challenge because of the functional importance and complex multidimensional structure of the facial units that are involved, and is most commonly found in developing countries. Therefore, few studies have been conducted on NUS. Moreover, reconstruction options vary from local regional flaps to free-tissue transfers. We report a very interesting case in which we performed regional flap surgery using bilateral cheek advancement in a patient with NUS. A 75-year-old woman with a history of diabetes mellitus and hypertension, but no other immunological diseases, presented with skin necrosis on the upper lip. At presentation, necrotic tissue covered the upper lip and philtrum, but it had not invaded the nose or lower lip. After debridement of the necrotic tissue, approximately 70% of the upper lip was missing. We therefore designed a bilateral cheek advancement and rotation flap, in which the flap was sutured in 3 layers. There was no need to perform additional procedures, as the flap healed well and showed no other complications or recurrence. The patient exhibited good voluntary muscle control and oral competence while eating and drinking, and she was also very satisfied with the cosmetic results. Thus, regional flap surgery using a simple advancement flap may result in good recovery of both functional and aesthetic units in patients with NUS.
INTRODUCTION
Necrotizing ulcerative stomatitis (NUS), also called “noma” (from the Greek word nome, meaning a pastureland for grazing), is often considered a rare disease, but it is commonly found in malnourished or unhygienic children in developing countries [1]. Its etiology is not completely understood, but one possibility is that malnourishment, unhygienic conditions, and immune system complications might lead to multibacterial facial gangrene [2,3]. Some of the recognized predisposing factors for this gangrenous orofacial disease involve mucosal and systemic immunosuppression, such as poor oral hygiene, inadequate protein consumption, vitamin deficiencies, poverty, and infections, including malaria, human immunodeficiency virus (HIV), and measles. While noma is difficult to treat in developing countries and is often associated with high mortality rates, it is a reconstructive challenge in developed countries, rather than a matter of survival. Central noma is associated with defects of the upper lip and nasomaxillary region, which contain cartilaginous structures and soft tissue. Because of the functional importance and complex multidimensional structure of the involved facial units, central noma, especially on the upper lip, is a reconstructive challenge. Historically, the surgical options have varied from local regional flap transfer, such as the Karapandzic and Webster flaps, to free flap transfer, such as forearm fasciocutaneous flaps, which are often needed when there are extensive defects, especially on the lip [4]. We report a case in which noma involving the upper lip was managed with a bilateral cheek advancement and rotation flap. Our technique could be an alternative for the reconstruction of relatively large defects of the upper lip, as it minimizes the disadvantage of microstomia, thereby promoting optimal aesthetic and functional outcomes.
CASE REPORT
A 75-year-old woman presented to our hospital with skin necrosis on the upper lip (Fig. 1) and a 7-day history of lip swelling. She had a medical history of diabetes mellitus and hypertension, but no other immunological diseases. A wound culture revealed Klebsiella pneumoniae infection. She had a C-reactive protein concentration of 0.86 mg/dL (normal range, 0–0.5 mg/dL), an erythrocyte sedimentation rate of 87 mm/h (normal range, 0–43 mm/h), a glucose level of 411 mg/dL (normal range, 60–108 mg/dL), and a glycosylated hemoglobin level of 13.5% (normal range, 4–6%). Her total protein and albumin levels were abnormally low, at 5.9 g/dL (normal range, 6.6–8.0 g/dL) and 3.1 g/dL (normal range, 3.3–5.2 g/dL). While being hydrated, the patient was admitted and intravenous cephalosporin for a presumed infection was started. She tested negative for HIV infection, and no other immune deficiencies were found upon further investigation. We thus concluded that the patient had NUS, given her background of diabetes mellitus, malnutrition, and poor oral hygiene. Treatment included daily wound dressing and chlorhexidine and hydrogen peroxide mouthwashes.

The patient presented with necrotic tissue involving approximately 70% of the upper lip. A wound culture revealed Klebsiella pneumoniae infection.
At admission, necrotic tissue covered the patient’s upper lip and philtrum, but it had not invaded the nose and lower lip. After we completed debridement of the necrotic tissue, approximately 70% of the upper lip was missing. Three days later, the premaxillary bone was exposed, but there was no sign of infection (Fig. 2). We then designed a bilateral cheek advancement and rotation flap using a vertical incision line near the perialar area that was shorter than is commonly used and an elongated transverse line along the nasolabial fold (Fig. 3). After local flap elevation, bilateral advancement and caudal rotation were performed. The skin on the philtrum was trimmed, and the flap was sutured in the mucosal, muscular, and skin layers (Fig. 4). In the muscular layer, we used vest-on-pants sutures. After dissection, the ends of the orbicularis oris muscle were easily sutured and, as there was no ‘dog ear’ with this modified technique, it was not necessary to remove redundant skin. There was no need to perform additional procedures, as the flap healed well and showed no complications or recurrence. No complaints of any functional problems, such as issues with pronunciation or mastication, were reported by the patient. At a 2-year follow-up, she was more comfortable and satisfied with both the aesthetic and functional results (Fig. 5).

A preoperative photograph taken 3 days after local debridement shows upper lip defects and premaxillary bone exposure.
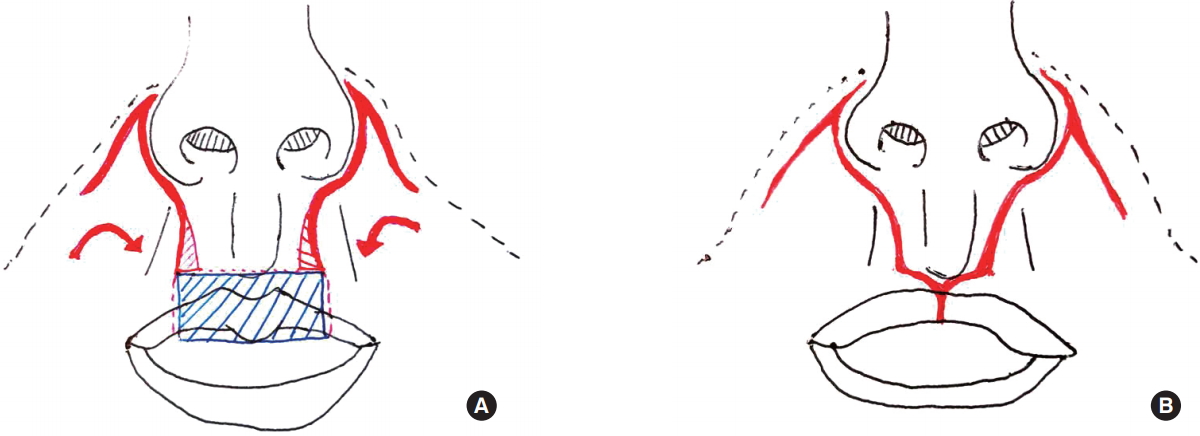
(A) Schematic illustration showing the preoperative design with the central upper lip defect. (B) Schematic illustration of the postoperative view.

Bilateral cheek advancement and rotation flap design (A). The flap was advanced medially and sutured in 3 layers (B).

A postoperative photograph taken 22 months after the flap operation shows good aesthetic results.
DISCUSSION
NUS is often considered a reconstructive challenge because of the involvement of complex functional and aesthetic units [4,5]. Also known as noma or cancrum oris, NUS is rare in developed countries and is more commonly encountered in malnourished children in developing countries. Cases are rarely reported in adults, but such cases are often associated with coexistent diabetes mellitus, leukemia, or HIV infection [6]. The pathogenesis of noma involves a high concentration of normal microorganisms in the mouth, which break down the resistance of a failing immune system. This condition leads to a spreading gangrene that quickly invades the facial tissues, leading to severe facial disfigurement, ankylosis of the temporomandibular joint, oral incontinence, and speech-related problems. If treatment is not administered in a timely manner, rapid tissue destruction follows, which then leads to devastating facial defects and a high mortality rate. Early diagnosis and intervention with local debridement, better oral hygiene, systemic antibiotics, and nutritional support can help reduce the rates of mortality, fibrosis, and oral disfigurement. As NUS has been considered a reconstructive challenge because it affects complex functional and aesthetic units [3,4,7] and because it is often found only in developing countries, few studies have investigated NUS. Options for reconstruction range from local regional flap transfer to free tissue transfer. The aims of lip reconstruction should be to maintain oral competence, a maximum oral aperture, mobility, sensation when possible, and cosmetic appearance.
By cheek advancement with a crescentic perialar excision flap, we performed single-stage reconstruction of a defect located in the subtotal upper lip. The main shortcoming of conventional flaps, such as the Karapandzic flap, is greater rounding of the commissure area. In addition, for better results, some adjacent normal tissue, such as a ‘dog ear’ and Burrow triangles, must be excised when fabricating the Karapandzic flap. Traditionally, when designing such a flap, an incision line is made near the ala to the perialar region. However, in this case, our flap design involved a shorter incision in the perialar region and an elongated incision along the nasolabial fold, which made the scar less visible.
By obtaining more tissue from the nasolabial fold region, we avoided rounding of the commissure and preserved the innervation and blood supply of the orbicularis oris muscle. This modification also allowed us not to excise Burrow triangles laterally, even when the tissue discrepancy was not resolved over the course of the semicircular incision for the Karapandzic flap. No microstomia was observed, and the patient did not complain of articulation problems or denture usage difficulties. Although the volume of the philtral column was reduced, there was no sign of destruction or functional discomfort. Subsequent volume replacement techniques, such as fat injection, could improve the tightened volume, and this procedure also had the advantage of being a single-stage procedure. In the case presented here, this flap provided sufficient resurfacing of large central upper lip defects with skin from the cheek.
A limitation of this flap is the shortening of the gingivobuccal sulcus and notching of the suture site of the upper lip. However, the use of a bilateral cheek advancement and rotation flap allowed a good color match and safe and reliable reconstruction of the affected area without causing additional rounding of the commissure or requiring the excision of adjacent normal tissue. Our experience confirms that this flap is a good option when considering the reconstruction of defects involving central upper lip loss.
Notes
No potential conflict of interest relevant to this article was reported.
PATIENT CONSENT
Patient provided written consent for the use of her images.