Local Subcutaneous Injection of Erythropoietin Might Improve Fat Graft Survival, Whereas Continuous Infusion Using an Osmotic Pump Device Was Harmful by Provoking an Overwhelming Foreign Body Reaction in a Nude Mouse Model
Article information
Abstract
Background
Since the survival of grafted fat requires successful revascularization, we hypothesized that local delivery of erythropoietin (EPO), a hemangiogenic and antiapoptotic factor, might enhance the survival of fat grafts in a nude mouse model.
Methods
Our experiment consisted of 2 parts. The first involved direct injection of EPO or saline at the grafting site before fat grafting and for 4 days afterwards. In the second part, EPO or saline was delivered continuously for 1 week via an osmotic pump device, and a group without an implantable pump represented the control group. After 16 weeks, the surviving fat grafts were weighed and subjected to histomorphometry.
Results
In the first experiment, fat graft survival was higher in the EPO-injected group, but not statistically significant (69.2% vs. 59.2%; P=0.21). Histomorphometry showed significantly higher levels of microvessel formation and less cystic degeneration in the EPO-injected group. In the second experiment, the survival rate was significantly lower in both pump groups than in the control group (40.7% in the EPO pump group, 7.7% in the saline pump group, and 66.7% in the control group).
Conclusions
Local injection of EPO into the fat graft site appeared to improve graft survival, with increased angiogenesis, suppressed inflammation, and decreased degeneration. However, the insertion of an osmotic pump exerted detrimental effects on graft survival and the histomorphometric profiles of the fat graft compared with the control group due to the overwhelming foreign body reaction.
INTRODUCTION
Free fat injection has become a common practice for various types of soft tissue augmentation, and its new role as a driving force in tissue regeneration has been described in recent publications [1,2]. However, inconsistency in long-term outcomes remains a drawback and there is no universal agreement on the best methodology or the necessary amount of overcorrection when performing a free fat injection [3-5].
The survival of grafted fat requires successful revascularization. A study of mice treated with an angiogenesis inhibitor demonstrated that the degree of revascularization determined the volume retention and influenced gene expression [6]. Other studies have attempted, with varying degrees of success, to augment graft survival using various growth factors, cytokines, or platelet-rich plasma (PRP) [7-11]. An increasing number of studies have implanted fat particles mixed with adipose-derived stem cells (ASCs) with promising results [12,13]. However, bedside application of this method seems unlikely in the near future due to excessive costs and other clinical safety issues.
Erythropoietin (EPO) is a potent hemangiogenic factor that, with the ubiquitous expression of its receptor, has been associated with diverse biological functions in various organs and tissues [14]. EPO is already widely used clinically, so its use in novel clinical applications seems somewhat more practical than the use of growth factors, PRP, or ASCs. Several reports have focused the role of EPO in angiogenesis and wound healing, with promising results [15]. Recently, its possible positive role in lipofilling was also investigated in an in vitro model [16]. Considering its proangiogenic and antiapoptotic effects, we hypothesized that local delivery of EPO might enhance the survival of fat grafts in a nude mouse model.
METHODS
Study design
Our experiment consisted of 2 parts. In the first experiment, we performed daily local injections of EPO at the graft site immediately before fat grafting and for 4 consecutive days afterwards. In the second experiment, we inserted an osmotic pump at the graft site for continuous delivery of EPO to the grafted fat, for a longer period of time with a larger dose. All aspects of the protocol were approved by the Institutional Animal Care and Use Committee of Asan Institute for Life Sciences (2009-13-063). Additionally, all institutional and national guidelines for the care and use of laboratory animals were followed.
Fat harvesting and processing
Fat was obtained from the mid-abdomen of 2 healthy anonymized donors (44 and 46 years in age) who underwent elective abdominoplasty. Informed consent was obtained from each donor using an Institutional Review Board-approved protocol. Harvested fat was centrifuged at 3,000 rpm for 3 minutes, and the middle centrifugation layer was transferred to a 1-mL Luer-Lok syringe. The weight of each aliquot was calculated by subtracting the weight of an empty syringe from the total weight of the syringe containing fat.
Animal model
Thirty-six week-old CD-1 male nude mice (weight, 20–25 g) were used in this study. The animals were kept under a constant laminar flow of air and allowed to feed ad libitum on standard laboratory chow and water. For transplantation, the animal weight was measured and 1 mL of fat was then injected into the subdermal scalp, using a sharp 16 gauge needles and spreading the fat through as large of an area as possible.
Part 1. Local injection of EPO
Eighteen mice were randomly divided into 2 experimental groups. Group 1E mice (n=9) were injected subcutaneously once daily with EPO (Epokine® prefilled injection; CJ Pharmaceuticals, Seoul, Korea) at a dose of 5,000 IU/kg for 4 days around the graft site (100 IU daily for a 20-g mouse, about 10 μL in volume) following fat injection. Group 1S mice (n=9) were administered an equal volume of sterile normal saline based on body weight. The first injection was performed 1 hour before fat transplantation at the site of the presumed graft bed for mice in both groups.
Part 2. Delivery of EPO via osmotic pump systems
Eighteen animals were randomly divided into 3 subgroups: notreatment control (group 2C, n=6), EPO delivered via an osmotic pump (ALZET® Model No. 1007D; ALZET Osmotic Pumps, Cupertino, CA, USA; group 2E, n=6), or sterile normal saline delivered via the same type of osmotic pump (group 2S, n=6). An osmotic pump containing 1,000 IU of EPO dissolved in 100 μL of normal saline was connected to a polyethylene catheter (inner diameter, 0.76 mm) and inserted in the subdermal lower back of the animal 1 hour before fat transplantation under anesthesia using 30 mg/kg of Zoletil (Zoletil®50; Virbac Inc., Carros, France) administered intraperitoneally. The end of the catheter was placed at the recipient site and fixed with a fast-absorbing suture (Fig. 1). This osmotic pump system allowed continuous delivery of EPO at a rate of 1 μL (10 IU of EPO) per hour (240 IU daily, for a total of 1,000 IU). The pump was surgically removed after 1 week through the back incision. A group without an osmotic pump served as the notreatment control group (group 2C, n=6).

Osmotic pump inserted into the grafted fat. The osmotic pump was connected to a polyethylene catheter and inserted in the subdermal lower back of the nude mouse. This osmotic pump system allowed continuous delivery of erythropoietin with a rate of 1 μL (10 IU of erythropoietin) per hour.
Data collection
All animals survived to the end of this study and were euthanized after 16 weeks following the study protocol. The surviving fat from the original graft was dissected, weighed, and reported as the percent weight (% weight) remaining from the initial injection weight. In cases where a macrocyst formed that contained necrotic material, the cyst portion, including the capsule, was excluded from the final weight measurement.
For the histological examinations, the central portion of dissected fat tissue was fixed in 4% formaldehyde, embedded in paraffin, and processed for hematoxylin and eosin staining. Five randomly selected fields from each slide were viewed by an independent observer to assess cellular integrity (the presence of nucleated fat cells), microvessel formation, cystic degeneration, fibrotic cicatrization, infiltration of inflammatory cells, and the presence of giant cells. Each parameter was graded on a semiquantitative scale (0–5) as follows: 0, absence; 1, minimal; 2, minimal to moderate; 3, moderate; 4, moderate to extensive; 5, extensive presence.
Statistical analysis
Statistical analyses were conducted using SPSS version 20.0 (IBM Corp., Armonk, NY, USA). Repeated measures 1-way analysis of variance and the Mann-Whitney test were used to compare the percent weight and histological parameters. P-values of less than 0.05 were considered to indicate statistical significance in general. For intergroup comparisons, P-values <0.01667 (0.05/3) were considered to indicate statistical significance, following application of the post hoc Bonferroni correction.
RESULTS
Part 1. Local injection of EPO
The average percent weight of surviving fat was 69.2% in the EPOinjected group (1E) and 59.2% in the saline-injected group (1S). Although fat graft survival was higher in the EPO-injected group, this tendency failed to reach statistical significance (P=0.21). All histological parameters were more favorable in the EPO-injected group (Table 1). Statistically significant differences were observed in microvessel formation and cystic degeneration (Fig. 2 and 3).
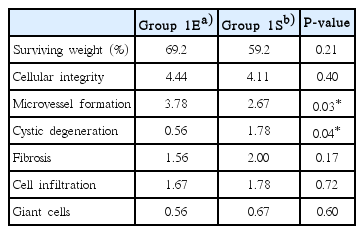
Comparison of graft survival and histomorphometric analysis results between group 1E and group 1S

Harvested fat from a mouse in group 1E. Surviving fat (arrows, viable adipocyte nucleus) with little degeneration and microvessel formation (arrowheads) were observed (hematoxylin and eosin stain [H&E], ×100).
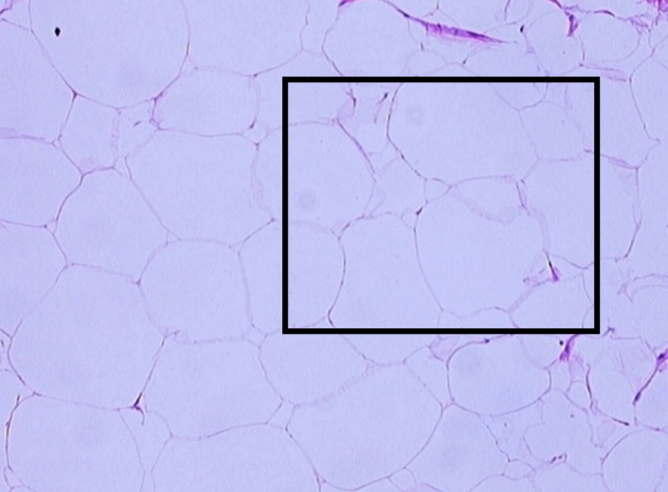
Harvested fat from a mouse in group 1S, showing microcystic degeneration. Less microvessel formation, with scattered fibrosis and cystic degeneration (box, ‘shadowy’ outlines without nucleus), was observed (hematoxylin and eosin stain [H&E], ×100).
Part 2. Delivery of EPO via an osmotic pump system
The average percent weight of surviving fat was 40.7%, 7.7%, and 66.7% in groups 2E, 2S, and 2C, respectively. When each pair of groups was compared, group 2E showed a significantly higher survival rate than group 2S (P<0.001). However, both group 2E and 2S group showed significantly poorer survival than the control group (group 2C; P<0.001, P<0.0001).
On histological evaluation, group 2E showed better overall results than group 2S, especially in terms of increased microvessel formation and fewer signs of inflammation. However, both osmotic pump groups (2E and 2S) showed a tendency for greater fibrosis and cellular infiltration than the control group (2C) (Table 2). Of note, group 2S consistently showed a notable level of fibrosis with macrocystic degeneration in the histomorphometric analysis (Fig. 4).

Comparison of graft survival and histomorphometric analysis results in groups 2E, 2S, and 2C

Harvested fat from a mouse in group 2S. The large adipose nodule represents macrocystic degeneration. Oil cysts were scattered in areas of fibrotic cicatrization (asterisks, examples of severe fibrosis) which displaced healthy fat tissue and extracellular matrix (hematoxylin and eosin stain [H&E], ×100).
DISCUSSION
The main disadvantage of free fat injection is its unpredictable absorption rate. Ischemia that occurs prior to revascularization of injected fat causes adipocyte degeneration, leading to macrophage recruitment and subsequent phagocytosis of cellular debris. Various proangiogenic factors and endothelial progenitor cells have been utilized in efforts to increase graft survival rates by enhancing the blood supply to the recipient area [8-10,17-20].
Although EPO is primarily known as a hemangiogenic factor, it plays a number of diverse biological roles in various organs and tissues, such as enhancing progenitor cell recruitment and inhibiting apoptosis. Animal studies have shown that EPO can protect against ischemia and reperfusion injury in various organs, including the heart, kidney, intestine, and liver [21-24]. EPO also promotes beneficial regeneration in neuronal tissue by enhancing progenitor cell recruitment and revascularization in injured regions [25,26]. This multifunctional factor has also been reported to enhance revascularization in an ischemic rat random flap and to increase survival in another rat random flap model [27,28].
A recent in vitro study reported that EPO affected the inflammatory response by reducing the number of macrophages [16]. It also has anti-inflammatory and antioxidant properties, similarly to dimethyl sulfoxide, which showed beneficial effects on the survival and volume preservation of fat grafts [29,30].
Hamed et al. [31] reported beneficial effects of pre- and subsequent treatment of EPO on the survival of grafted fat, and they claimed that the effect was even more potent than that of vascular endothelial growth factor. EPO treatment also increased the expression of angiogenic factors and microvascular density, and reduced inflammation and apoptosis [31]. These results are associated with both local and systemic effects, since subcutaneous injection of EPO in hemodialysis patients is known to be associated with more favorable clinical outcomes than intravenous treatment [32]. Based on these prior reports, we first tried to enhance the survival of fat grafts using local subcutaneous injections of highdose EPO (5,000 IU/kg per treatment) at the graft site, with a shorter treatment period (5 perioperative days vs. 18 days) in our first experiment. A trend towards a better histomorphometric profile was observed, as indicated by significantly increased microvessel formation and less cystic degeneration, which led to a tendency towards a higher survival rate than the saline-injected group, but the difference in fat graft survival was not significant.
However, in regenerative medicine research using animal models, continuous regional infusion of EPO using an osmotic pump was associated with enhanced functional recovery after global cerebral ischemia and protective neurogenesis in a model of Parkinson disease [33,34]. These protective effects have been proposed to be associated with several mechanisms, including the prevention of apoptosis and the stimulation of trophic factors. As the results from the first experiment showed possible benefits of EPO for increased fat survival, we hypothesized that the beneficial effect of continuous regional infusion of EPO on the neuronal system might also occur in the grafted fat tissue.
However, our set-up with an osmotic pump produced completely opposite results, as EPO delivery via an osmotic pump caused a significant reduction in the surviving graft weight compared to the no-treatment control group. The animals that received saline via an osmotic pump showed an even more dramatic reduction in fat graft survival.
Upon histological evaluation, the animals that were treated with either EPO or normal saline via the pump showed a marked increase in inflammatory cell infiltration and fibrosis. The addition of EPO seemed to have exerted a beneficial effect via its potent anti-inflammatory effect, as reflected by improved graft survival and a more favorable histological profile than the saline group. However, an exaggerated inflammatory response caused by local stimulation by the catheter itself, as well as an enhanced systemic inflammatory reaction, led to increased macrophage accumulation and subsequent destruction of fat cells. Similar results have been reported after the administration of interleukin-8, a proinflammatory mediator, which led to an improved histopathologic profile without an increase in the survival rate [9]. Haifei et al. [35] observed that the foreign body reaction, as demonstrated by giant cell formation, was the most extensive in the thickest scaffold and that vessel formation was the greatest in the thinnest scaffold, with the assumption that an enhanced cytokine response would have played a role in the degradation process, underlining the implications of inflammation and foreign body reaction in graft survival.
According to Kato et al. [36], initially ‘dead’ adipocytes are replaced by next-generation adipocytes in favorable microenvironments. An excessive inflammatory reaction seems to expand the necrotizing zone and to shrink the regenerating zone because the acute inflammatory response involving cellular influx leads to cell and tissue damage and subsequent resorption by macrophages. When lipid replacement with scar tissue predominates, fibrosis occurs, further hindering adipose stem cell differentiation [37].
Although fat graft survival depends on revascularization, resorption of the graft is not solely dependent on the amount of blood supply. An exaggerated inflammatory response before complete revascularization may lead to significant resorption of the grafted fat and cicatrization, as in the current study. Similar results were recently published by Cai et al. [37] who reported that low-dose granulocyte colony-stimulating factor improved fat graft retention by mobilizing stem cells and inducing angiogenesis, whereas high doses inhibited adipogenesis, with prolonged inflammation and severe fibrosis. In short, fat graft survival requires an appropriate inflammatory response at the early stage to initiate precursor cell proliferation and angiogenesis, followed by quick remission to prevent excessive phagocytosis and fibrosis.
Although it failed to reach statistical significance, we showed some possible benefits of EPO, and more importantly, the significantly detrimental effect of excessive or prolonged inflammation on the survival of fat grafts. Future studies on the effects of beneficial agents or growth factors should employ a benign delivery method such as direct injection, mixing with the graft, or the use of microspheres, as reported by previous studies [38,39]. In clinical practice, the principle of minimizing the inflammatory reaction should be considered when fat grafting is performed with other procedures, especially when an alloplastic material or prosthesis is being concurrently implanted.
Notes
No potential conflict of interest relevant to this article was reported.