INTRODUCTION
A supernumerary nipple is a common minor congenital malformation that consists of accessory nipples or related tissue in addition to the nipples normally appearing on the chest; it can appear on the chest or along the two vertical milk lines which start in the armpit on each side, run down through the typical nipples and end at the groin. They are believed to arise from the persistence of ectodermal ridges that normally regress during intrauterine development. They are classified into eight types by Kajava (Table 1). Polythelia refers to the presence of an additional nipple alone without any glandular, areola or fat tissue, and it is the most common type.
The prevalence of supernumerary nipples is estimated to be 1 in 500 (0.2%) [1]. They are usually asymptomatic and undetected, but occasionally become apparent during puberty, menstruation, or pregnancy when hormonal changes result in increased pigmentation, swelling, tenderness, or even lactation.
Although supernumerary nipples are relatively common, intraareolar polythelia (IAP) is an extremely rare congenital malformation, and there are only ten cases in the literature [2]. Surgical excision is indicated for diagnostic, treatment, or cosmetic problems. The authors report a case of extremely rare IAP of a young female patient on her right breast.
CASE REPORT
A 24-year-old female patient visited our clinic with a small protruding accessory nipple (3 mm×4 mm in size) next to her right nipple inside the areola on the right breast (Fig. 1). The size of the right breast and its areola was normal and similar to the left breast. She had had the accessory nipple since she was 5 or 6 years old, and it enlarged 3 to 4 years before presentation to our clinic.
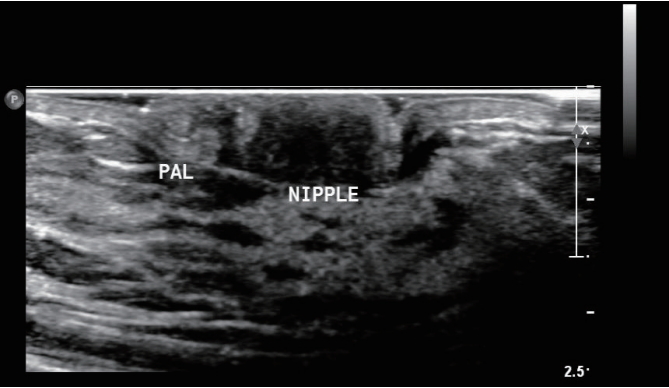
There was no specific medical history which might relevant to the lesion, and physical examination showed neither pain nor tenderness. Breast ultrasonography revealed no abnormal finding in either breast, and the lesion had similar structures to ordinary nipples (Fig. 2).
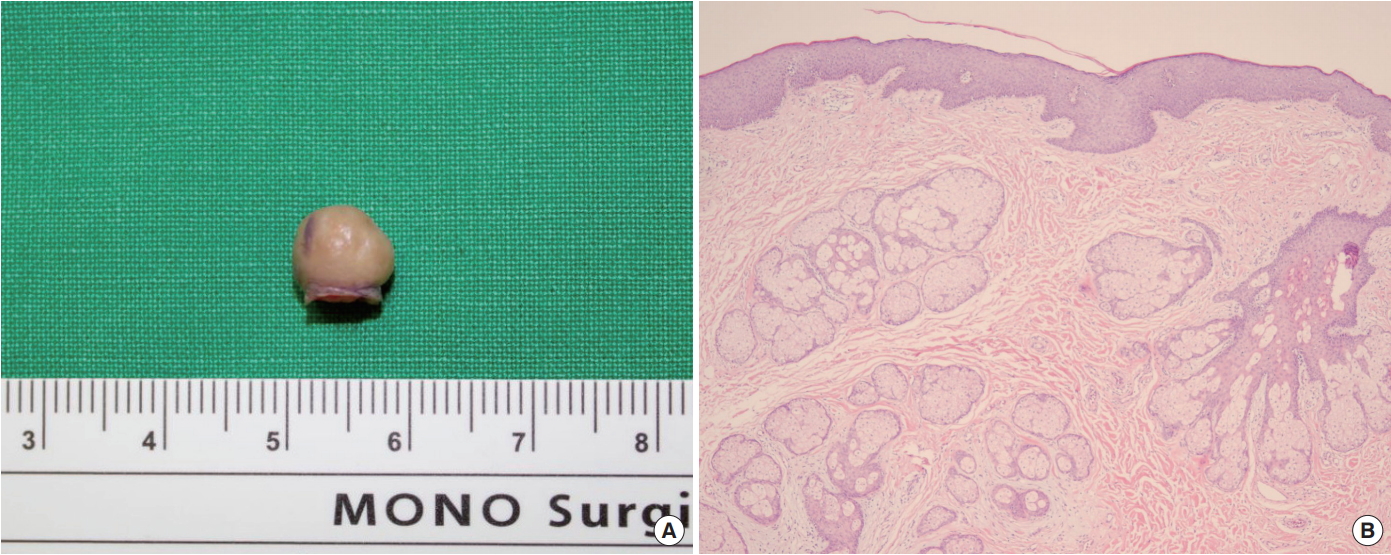
In order to prevent postoperative deformity, minor S-plasty was performed on the accessory nipple for surgical excision under local anesthesia; biopsy was also performed (Fig. 3). The histological findings of the excised nipple (Fig. 4) were consistent with normal nipple tissue without any glandular or areola tissue. Diagnosis of the accessory nipple was made as supernumerary nipple Type VI based on the Kajava classification. There were no complications after the operation.
DISCUSSION
While a supernumerary nipple is a relatively common anomaly, IAP is extremely rare. Ordinarily, supernumerary nipples normally appear along the two vertical milk lines. During the fourth week of gestation, paired ectodermal thickenings known as “mammary ridges” or “milk lines” develop. In normal human development, these ridges disappear except at the level of the fourth intercostal space on the anterior thorax where the mammary gland subsequently develops. It is believed that polythelia results from the persistence of ectodermal ridges along the milk lines, which normally regress during intrauterine development. The remnant may evolve into a complete mammary gland, resulting in the condition known as polymastia or a small remnant as polythelia or accessory nipple. Approximately 67% of accessory breast tissue occurs in the thoracic or abdominal portions of the milk lines, while 13% occurs in the axillary area [3]. Unlike ordinary accessory nipples, IAP is an extremely rare congenital malformation. Only ten cases have been reported in the literature [2].
No detailed surgical treatment guidelines have been established for correction of this rare congenital malformation. However, it is believed that a correlation exists between polythelia and renal diseases such as cysts, duplications, or unilateral renal agenesis [4] and also with malignancy changes in 5% of polythelia cases [5]. For this reason, the treatment of choice should be surgical excision as prophylaxis against breast cancer and cosmetic problems.