INTRODUCTION
Applying external fixators or distractors is a common method used to manage complex fractures [1]. Although good alignment and bony union are important, prolonged pin placement may cause epidermal ingrowth and tethering of soft tissues to the underlying bone [2]. These can result in retracted and depressed scars in the site where the pins passed through the skin, and these scars do not resolve or improve spontaneously [1-5]. Several methods have been introduced to manage these scars [3-5]. A surgical method combining W-plasty and a buried dermal island was introduced in 1994 [4,6]. Subsequently, a procedure involving blind dissection under the scar tissue using sharp scissors with a 1-cm longitudinal incision was introduced [5]. In another study, it was found to be possible to improve the appearance of a pin-site scar by performing subcisions with a 16-gauge needle and fat injections [3]. However, if these methods do not resolve a scar, it may be necessary to try another method.
Acellular dermal matrix (ADM) has been used for soft tissue replacement in skin grafts, facial augmentations, and other reconstruction procedures [7,8]. The implantation of ADM can enable much of the original augmented volume to be retained over time, making it useful for volume replacement procedures [7-9]. Therefore, we describe a case of pin-site scars that resolved after use of an effective method based on ADM implantation and subcisions.
CASE REPORT
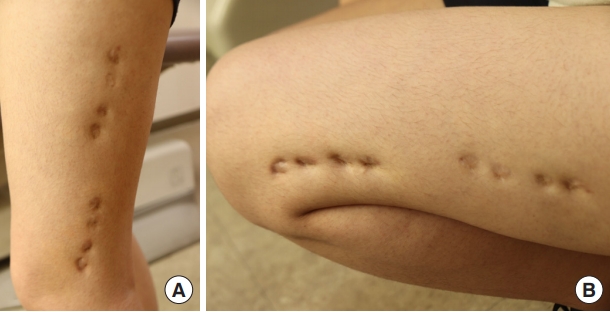
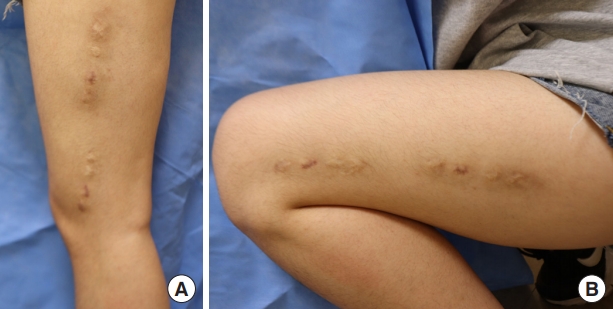
An 18-year-old Asian woman presented with multiple dimpled scars on her left thigh. She had a distal femur fracture on the left side at the age of 6 years and underwent external fixation at that time. She had eight scars along the vastus lateralis muscle, each of which was 1 cm in size. With a depression of 0.5 cm in the standing position, the scars worsened when her knee was bent. Although we performed an autograft fat injection at the sites of the scars, the scars remained depressed (Fig. 1). Therefore, 6 months after the first operation with a fat injection, we planned to use an ADM to supplement the soft tissue and to enhance the dermal layer. The incisions were made in the center of the scarred region (with four consecutive scars on each side), providing easy access to the surrounding tissues and leaving no additional scars. The use of zig-zag incisions enabled a wider field of view to be used, and the resultant scar was less noticeable than the linear scars after the operation (Fig. 2). Blunt subcutaneous undermining was performed with Metzenbaum scissors to break up the fibrous bands that caused the depressions. Subcutaneous dissection was extended step-by-step under close observation to avoid injuring the dermal layers. Sufficient elevation of the scars was done gradually and a freely movable flap was visually confirmed. With sufficient dissection, two ADMs measuring 1×4×0.1 cm (AlloDerm; LifeCell Corp., Branchburg, NJ, USA) were inserted through each incision. Using Prolene #3-0, pullout stitches without knots were used to locate each ADM under the skin flap, and wound closure tape (Steri-Strip; 3M, Maplewood, MN, USA) was applied to the skin to stabilize the ADMs (Fig. 2). The pullout threads were removed on postoperative day 7, and the stitches were removed from the incision site on postoperative day 13. Prior depressions caused by bending of the knee could not be observed in any positions taken by the patient (Fig. 3). One month after the operation, treatment with an Erbium glass fiber laser (MOSAIC HP; Lutronic, Goyang, Korea) was administered to improve the scars.
DISCUSSION
Although scar formation is an inevitable consequence of wound healing, it can have a significant impact on patients’ physical and psychological well-being [10]. The ideal scar is directed along a relaxed skin tension line, is thin and flat, and matches well with the surrounding skin [6]. In clinical practice, many scars are symptomatic, unsightly, and not ideally oriented with the skin [6,11]. Especially in scars resulting from external fixation, prolonged pin placement can cause skin pressure or pin tract infections, leading to fibrotic and depressed scars on the pin-fixed site [3-5].
To manage scars induced by external fixation, adequate undermining of the soft tissues and volume replacement are needed. It is important to perform enough subcisions of the adhesions and fibrotic tissues under the scar because scars resulting from the percutaneous placement of transosseous pins or wires are hard to release [1,3].
In our case, we thought that scar revision with linear excision could increase the length of the scars and that muscle movement may cause the scars to be hypertrophic [6,10,11]. Autologous fat grafting is a treatment option, but the results can be unsatisfactory because the graft survival rate ranges from only 40% to 80% [12]. Although new approaches to fat grafting have been developed to improve the survival rate, the collection of fat tissues is still complicated, a large amount of time is still required, and problems related to reabsorption remain [12]. To avoid the need for tissue transplantation from a donor site, a potential alternative in which biomaterials facilitate tissue regeneration in the defect area has been developed [7,9,13]. Among the materials used, the extracellular matrix has been proven to be useful as a scaffold for tissue reconstruction and volume replacement [7-9]. Therefore, the use of ADM is another option for treating external fixation scars, such as those encountered in our case.
The use of a fat graft before surgery in our case might have improved the circulation around the scars [12]; however, it was not as effective as ADM insertion. This may be due to the different physical properties of fat and ADM. Considering the physical characteristics of the scaffolds used in tissue engineering, ADM presents higher tensile stress than other biological materials, including human fat [14,15]. This may have contributed to the stable reshaping of the pin-site scars when ADM was inserted in the depressed area and to the enhancement of the dermal layer, keeping the skin from returning to its original site.
Scar revision procedures have the potential to improve patients’ quality of life by creating scars with better tissue quality that are cosmetically and functionally more acceptable. Although more cases and studies are needed, this case shows that scar revision with an ADM can be useful for dimpled scars such as pin-site scars.