Psychological characteristics of adult neurofibromatosis type 1 patients seeking elective surgery
Article information

Abstract
Background
Neurofibromatosis type 1 (NF1) is an autosomal dominant genetic disorder involving the nervous system characterized by the development of neurofibromas throughout the body. Patients with NF1 are also known to have cognitive, behavioral, social, and emotional problems. Using the Symptom Checklist-90-Revision (SCL-90-R) questionnaire, we aimed to assess the psychological characteristics of NF1 patients seeking surgery at a tertiary hospital.
Methods
Adult NF1 patients visiting a plastic surgery outpatient clinic between March 2018 and March 2020 were enrolled in this study. The presence and intensity of psychopathological symptoms were assessed using 10 domains, including the General Severity Index (GSI). Standard T-scores were used to compare the results to population-based norms. The impact of demographic factors was also analyzed.
Results
In total, 65 patients were included in the study. The mean GSI of all patients was 43.7, and the mean score of the other nine domains was 45.3. No scores deviated from the population-based normal ranges. Nonetheless, women had significantly higher mean T-scores than men in a few domains, including the GSI, obsessive-compulsive disorder, depression, and anxiety. Most of the other characteristics, such as age, education, marital status, family history, and tumor site did not have significant effects.
Conclusions
Adult NF1 patients who visit plastic surgery clinics for elective surgery have psychopathological characteristics that do not differ from the general population according to the SCL-90-R. The results of this study can be considered in consultations with these patients.
INTRODUCTION
Neurofibromatosis type 1 (NF1) is an autosomal dominant genetic disorder involving the nervous system, caused by a heterozygous mutation of the NF1 tumor suppressor gene on chromosome 17. It affects approximately 1 in 2,500 to 3,000 individuals, with an equal sex distribution [1]. As implied by the name of the disease, neurofibroma development is one of its major clinical features. Neurofibromas are tumors of peripheral nerve sheath origin. They can appear in any part of the body, with variable clinical and pathological manifestations. Generally, their presentations range from the most common localized forms to complex diffuse or plexiform types [2]. Moreover, a rare malignant form also exists, characterized by tumors known as malignant peripheral nerve sheath tumors. Otherwise, neurofibromas are basically benign tumors, although they can arise virtually anywhere that nervous tissue exists and cause sensory or motor symptoms. In some cases, significant morbidity or even death occurs, depending on the location or tumor burden. Even in cases without considerable morbidity, the disfigurement caused by multiple cutaneous neurofibromas or a few huge plexiform neurofibromas can cause profound distress to the individuals affected.
As for the cognitive and emotional aspects of NF1, it has been reported that children and adolescents with NF1 present with significant alterations in language skills, motor function, executive function, attention, behavior, emotion, and social skills. A high prevalence of attention-deficit/hyperactivity disorder, autistic traits, and autistic spectrum disorder have also been reported in association with NF1 [3,4]. Compared with unaffected children and adolescents in the general population, pediatric and adolescent patients with NF1 have an increased risk of exhibiting social difficulties, mental health disorders, and behavioral and emotional problems, as well as a diminished quality of life (QOL) [5]. In a cross-sectional study by Cohen et al. [6], 55% of adult NF1 patients likely had clinical depression.
The main objective of this study was to assess, using the Symptom Checklist-90-Revision (SCL-90-R), the psychological characteristics of NF1 patients seeking plastic surgery at a tertiary hospital. Furthermore, the impact of various factors, such as sex, age, education, family history, and tumor location was analyzed.
METHODS
This cross-sectional study included NF1 patients visiting a plastic surgery outpatient clinic at a tertiary hospital in Korea between March 2018 and March 2020. Eligible patients were ≥18 years old, had already received or intended to undergo surgery for benign neurofibromas, and had completed the SCL-90-R questionnaire. This study was approved by the hospital’s institutional review board (2019-1462). The presence and intensity of psychopathological symptoms were assessed using the SCL-90-R, which covers nine primary symptom dimensions: somatization, obsessive-compulsive disorder, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. The SCL-90-R comprises 90 items, which are scored on a scale from 0 to 4 (0, not at all; 1, a little bit; 2, moderately; 3, quite a bit; and 4, extremely). To assess the clinical relevance of the findings, the SCL-90-R scores were converted to standard T-scores (ranging from 30 to 80) by referring to the appropriate population-based norm tables provided by the test manual. A T-score of 50 represents the mean T-score of the general population, and T-scores ranging from 40 to 60 represent the normal range (as defined by mean±standard deviation). A T-score of 63 corresponds to the 90th percentile and is clinically meaningful; a T-score of 55 is considered relatively high. Table 1 presents definitions of the psychopathological symptoms and disorders measured by the SCL-90-R [7,8].

Description of subscales in the Symptom Checklist-90-Revision (SCL-90-R)
Statistical analyses were performed using SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, NY, USA). The two-sample t-test was conducted to assess differences between two independent groups. For three-group comparisons, analysis of variation was performed to evaluate the statistical significance of differences between means. Statistical significance was confirmed by P-values <0.05. The psychopathological characteristics of the entire patient group were analyzed and compared with the population-based norms using standardized T-scores with no control group.
RESULTS
In total, 65 patients completed the SCL-90-R questionnaire. The mean T-score for all patients was 43.7±11.7, which was within the normal range, and no subscales deviated from the population-based norms (Table 2).
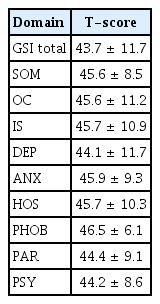
Overall T-scores (n=65)
Women had a significantly higher mean General Severity Index (GSI) T-score (45.37±12.86) than men (41.80±9.78; P=0.027). Moreover, women had significantly higher mean T-scores than men for the dimensions dealing with obsessive-compulsive disorder (P=0.023), depression (P=0.012), and anxiety (P=0.027) (Table 3).

Comparison by sex
Older patients had higher mean T-scores than younger patients (49.20±8.10 for age ≥50 years vs. 41.25±12.68 for patients in their 20s) (Table 4). However, no statistically significant correlations were found between age and T-scores for any of the categories that were analyzed (Tables 4, 5).

Comparisons by age

Correlation coefficients according to age
The mean T-score among patients with a high school diploma-level education (42.29±13.40) was similar to that of patients who graduated from college (43.50±10.45). In contrast, the mean T-score among patients who had less than a high school diploma-level education (47.60±8.79) was higher than those of the other two education-level groups, but these differences were not statistically significant (P=0.628) (Table 6).
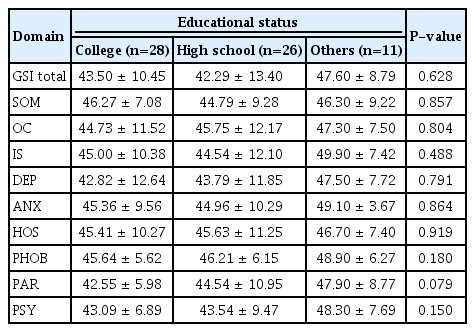
Comparisons by educational status
Married patients had higher mean T-scores than unmarried patients for depression (45.60±9.28 vs. 43.45±12.50, respectively; P=0.929) and paranoid ideation (45.90±7.47 vs. 43.75±9.61, respectively; P=0.916). For hostility, married patients (44.60±8.91) had lower meant T-scores than unmarried patients (46.20±10.81, P=0.361). None of these differences were statistically significant (Table 7).

Comparisons by marital status
Among the patients who answered the questionnaire, those with a family history of NF1 scored lower than those without a family history, except for somatization. Hostility was the only category for which family history was associated with a significant difference in mean T-scores (family-history group, 42.90±7.57; no-family-history group, 48.20±11.68; P=0.042) (Table 8).

Comparisons by family history of neurofibromatosis 1
Lastly, patients with tumors on the face and neck had higher mean T-scores for obsessive-compulsive disorder (face and neck, 48.32±11.72; extremity, 44.06±7.58; trunk, 42.80±12.40), interpersonal sensitivity (face and neck, 48.24±11.41; extremity, 42.94±8.00, trunk, 44.30±11.90), depression, anxiety, and hostility. Using the two-sample t-test, it was found that patients with face and neck tumors had significantly higher mean T-scores for depression (P=0.03) and hostility (P=0.047) than patients with tumors affecting other body sites. The differences associated with obsessive-compulsive disorder (P=0.051) and anxiety (P=0.074) score were marginally significant, and the differences associated with the other analyzed symptoms and disorders were not statistically significant (Table 9).
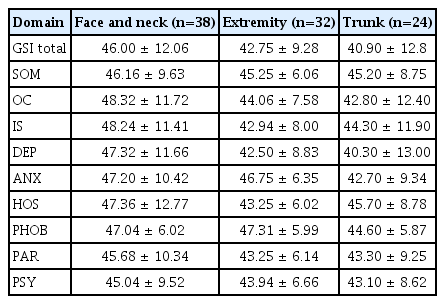
Comparisons by the main bodily region of the disease
DISCUSSION
The SCL-90-R is a self-report mental health questionnaire mainly used to evaluate a patient’s psychological state. It is short, easy to use, has been used in many studies, and the Korean-translated version is well established [7-9]. The reliability and validity of the SCL-90-R has been proven in various patient groups. This test has been used to interpret the causes and consequences of various diseases, since the questions are simple and can be applied to a wide range of patients [10-15]. When applying and interpreting the SCL-90-R, it is common to compare the scores of patients and controls, but the tool can also be used to compare patients’ scores with population-based norms using standard T-scores, an approach that has been utilized in other regions with their own population-based norms [16]. We analyzed the results using standardized T-scores based on Korean non-patient population data collected in 2014 from 1,000 normative people (501 males and 499 females) based on the population distribution by region and internet usage by age. Standard T-scores were also verified by age distribution and education level. A T-score of 63 corresponds to the 90th percentile and is clinically meaningful, and a T-score of 55 is considered relatively high. This enables within- and across-profile interpretation without a control group [17].
In general, it has been reported that NF1 patients commonly show neurodevelopmental abnormalities in various domains and to various degrees. For example, impairments in general cognitive/executive function, learning and social skills, anxiety and depression are associated with NF1 [4-6]. This is more than a social myth that comes from appearance, because these impairments are caused by pathogenic variants in genes encoding the Ras-mitogen-activated protein kinase signaling pathway [18]. These neurological and emotional features have significant negative impacts on QOL [19,20]. In the NF1 patient group of our study, however, there was no significant cognitive or emotional deviation relative to the general population. Except for sex, the demographic variables did not affect any of the SCL-90-R domains, including the GSI. Women are generally considered to be at a higher risk of mood disorders, even among non-neurofibromatosis patients. In fact, women have been reported to score higher in every subscale of the SCL-90-R except psychoticism (although the difference was not statistically significant for the psychoticism domain, as it was for somatization) [21], and Ablon [22] also described differences in responses to NF1 by sex, claiming that attitudes and social lifestyles, as well as the effects of changes in appearance on marriage or occupational outcomes, differ by sex.
Even considering these aspects, the results of our study significantly differed from those of previous publications. There are some important points to consider when interpreting the results. In terms of academic background, the majority of the study patients had at least an undergraduate-level education, and among the high school graduates, there were many current college students. Additionally, half of the unmarried patients were still young, in their 20s and 30s. This could be explained by selection bias, which is an intrinsic limitation of our study. In other words, among all individuals with NF1, our patients were those who visited a tertiary hospital for the purpose of surgery and who had the intellectual capacity and desire to fill out the questionnaire. This limits the generalizability of our results to all NF1 patients. Nonetheless, these patients are, broadly speaking, representative of the NF1 patients encountered at plastic surgery clinics.
A few studies have analyzed the relationship between QOL and the tumors themselves among NF1 patients. One study found that tumor burden was only correlated with pain, and not general QOL [23]. However, Granstrom et al. [24] claimed that adult NF1 patients had negative body image and less self-confidence, and that body image was an important link between disease visibility and psychological well-being. A similar perspective was also reflected by Taylor and Lewis [25], who asserted that surgery for NF1 is not cosmetic; rather, it is restoration of a normal appearance from disfigurement. However, considering the disease entity and the patient characteristics revealed by our results, elective surgery for NF1 is similar to aesthetic surgery in some respects. Therefore, when consulting with patients and deciding on surgery for NF1 (especially the cutaneous type), it is necessary to consider these issues and to clearly discuss the motivations for surgery, as well as its limitations.
The most important limitations of this study are that was based on a self-report questionnaire, making many of the findings subjective, and that there was inherent selection bias caused by enrolling only NF1 patients who visited a plastic surgery outpatient clinic at a tertiary hospital and who were able and willing to complete a questionnaire. The study would have been more comprehensive and objective if we had compared the patients to a non-patient group or another benign tumor patient group. Nevertheless, to our knowledge, this was the first study to describe the psychopathological features of selected NF1 patients seeking elective surgery.
In conclusion, according to the SCL-90-R findings, adult NF1 patients who voluntarily seek elective surgery have psychopathological characteristics that do not differ from the general population. Women had significantly higher mean T-scores than men in some domains, including the GSI, obsessive-compulsive disorder, depression, and anxiety, but all T-scores were within normal ranges. Features such as age, education, marital status, family history, and tumor site mostly did not have significant effects. These results should be considered when considering surgery for such patients.
Notes
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Institutional Review Board of Asan Medical Center (IRB No. 2019-1462) and performed in accordance with the principles of the Declaration of Helsinki.
Patient consent
The patients provided written informed consent for the publication.