INTRODUCTION
Facial defects have numerous causes, including skin cancer, trauma, and congenital malformations. Various methods exist to address these issues, with the chosen approach varying depending on the defect size and position [1-6]. Defects near vital structures such as the periorbital, perioral, and perialar areas must be reconstructed without any deformities, as deformities in these regions can cause functional and aesthetic problems [3]. The reconstruction of lower eyelid defects is prone to complications, such as ectropion and epiphora, and therefore requires caution [3]. Defects can be easily covered with grafts, but depression deformities can arise, and color differences with surrounding tissues may be present [6]. Rhomboid flaps are geometrically random pattern-designed fullthickness cutaneous transposition flaps. These flaps can cover defects with tissues of similar thickness and color, making them common choices for facial reconstruction [7]. However, rhomboid flaps also have disadvantages, such as the potential for tension, additional scarring, or dog-ear deformity [7]. Advancement flaps are also a popular reconstructive option, but they require long additional incisions for tension-free closure.
In this report, we introduce and analyze a sickle-shaped flap (a transposition flap) as a simple reconstructive method for the repair of small to moderate-sized lower eyelid defects.
METHODS
Patients and ethical approval
This investigation was reviewed and approved by the Institutional Review Board of Hanyang University Seoul Hospital (IRB No. 2020-06-018). A retrospective chart review was performed for all patients who underwent wide excision and reconstruction after skin cancer or trauma in 2018 or 2019. Of this larger group, patients who underwent reconstruction using a sickle-shaped local flap were included in the study. Tumor locations were limited to the medial canthal, lower eyelid, and lateral nose areas, presented as zones 1 and 2 in a previous article [8]. Patients with insufficient medical records or with a follow-up period of less than 1 year were excluded.
Surgical method
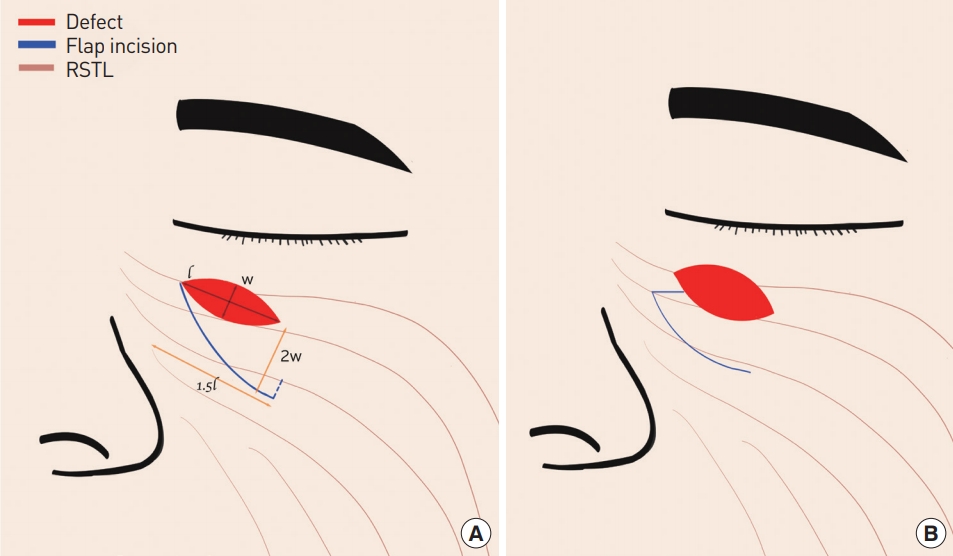
After wide excision of the skin cancer or debridement, the defect was measured. The width and length of the defect were the primary indicators for the flap design. The flap base was designed to be approximately twice the defectŌĆÖs width. The incision was started at the end of the defect and extended along the relaxed skin tension lines (RSTLs). The incision length was approximately 1.5 times the defect length. The defect was closed with the migrated flap, and dissection was then performed around the donor site. If the flap became subject to tension during donor site closure, non-absorbable sutures were placed between the deep structure and the lower flap to prevent traction of the recipient site (Fig. 1A). If the flap tip was too narrow or short to cover the defect, the tip was moved to a more distal point. This modification enabled coverage of the defect without tension (Fig. 1B).
Patient evaluation
Follow-up evaluations were performed every 3 months for 1 year and thereafter twice a year for an additional 2 years. Photographs were taken at every visit, and the Vancouver Scar Scale was used to evaluate residual marks every 3 months until 1 year postoperatively. Analysis of the photographs was performed by one of whom was the operator (SOP) and the other a third-year resident (THL). Patients reported their subjective satisfaction using a visual analogue scale ranging from 0 to 10 for the subcategories of pain, dry eye, erythema, edema, and ectropion, as well as their overall satisfaction at 1 year postoperatively.
RESULTS
A total of nine patients were included. The mean follow-up period was 18.39 months (range, 13.73ŌĆō26.03 months). The defect etiologies were basal cell carcinoma (7/9, 77.8%), squamous cell carcinoma (1/9, 11.1%), and trauma (1/9, 11.1%). The defects were measured along the long and short axes. The mean length of the long axis was 15.27 mm (range, 11.58ŌĆō19.29 mm) and that of the short axis was 8.46 mm (range, 6.18ŌĆō10.72 mm). The majority of the defects were located on the lower eyelid (6/9, 66.7%), followed by the medial canthal area (2/9, 22.2%) and the lateral nose (1/9, 11.1%) (Table 1).
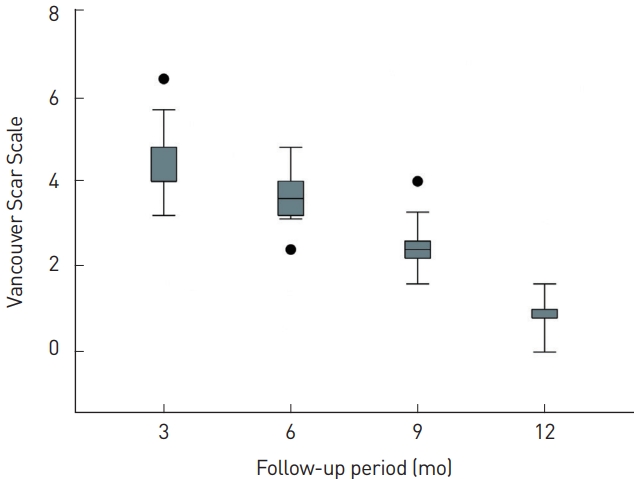
No flap necrosis, ectropion, epiphora, or other complications were observed. Among the eight patients with skin cancer, no recurrence was noted during the follow-up period. The mean Vancouver Scar Scale score was 5.50┬▒0.99 after 3 months, 4.61┬▒0.85 after 6 months, 3.05┬▒0.80 after 9 months, and 1.11┬▒0.58 after 1 year (Fig. 2). The mean overall patient satisfaction rating was 9.11┬▒0.78 (as rated on the visual analogue scale) (Table 2).
Case 1
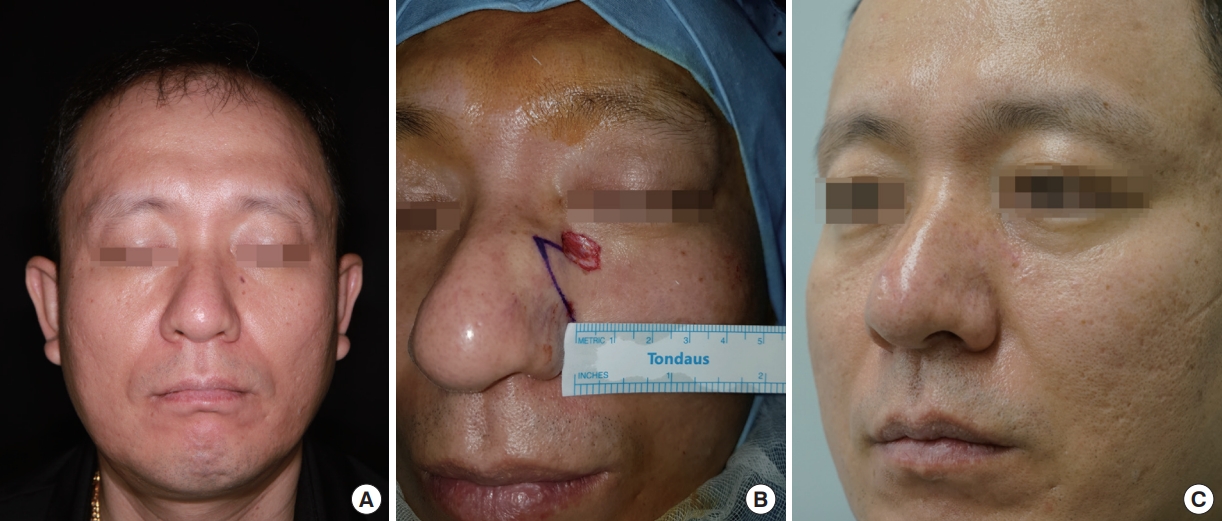
A 78-year-old woman was diagnosed with basal cell carcinoma of the right lower eyelid. Preoperatively, a punch biopsy was used to confirm a diagnosis of basal cell carcinoma, and the patient was referred to the plastic surgery department for wide excision. Excision was performed under local anesthesia, resulting in a 1.5├Ś0.6-cm oblique defect in the lower eyelid region. The incision was designed in an RSTL-oriented direction with a length of 2.5 cm, which was approximately 1.7 times the defect length. The flap base was 1.2 cm, approximately twice the defect width. Inferiorly, the lower lid was subject to slight tension, and temporary tarsorrhaphy was placed to prevent ectropion and removed on postoperative day 5. To prevent postoperative hematoma, a small Penrose drain was inserted; this was removed the day after surgery. At 12 months postoperatively, the Vancouver Scar Scale score was 2, and patient satisfaction as rated on the visual analogue scale was 9 (Fig. 3).
Case 2
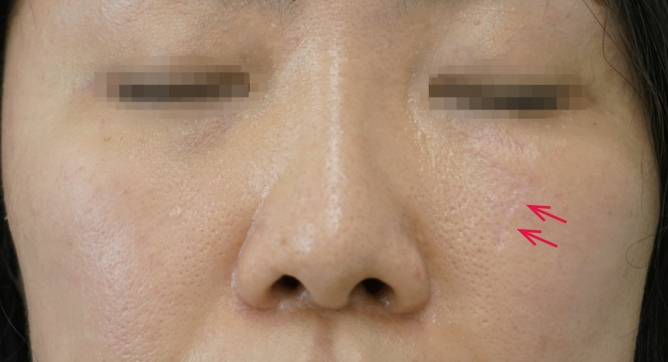
A 45-year-old man was diagnosed with basal cell carcinoma of the left lower eyelid. Wide excision was performed under local anesthesia, resulting in a 1.3├Ś1-cm defect on the medial side of the left lower eyelid. The defect was circular, with its longitudinal axis parallel to the RSTL. In such cases, a conventionally designed flap would have too narrow a tip, providing insufficient coverage of the defect. To address this concern, sufficient tissue can be secured using a modified method that moves the flap tip. This technique was utilized in this case, and no postoperative complications occurred. At 12 months postoperatively, the patientŌĆÖs Vancouver Scar Scale score was 1, and patient satisfaction was 10 as rated on the visual analogue scale (Fig. 4).
DISCUSSION
The face includes various sensory organs, the improper functioning of which impairs appropriate response to stimuli and decreases quality of life. The eyelid is the site of 5% to 10% of all skin cancers [9]. Complete remission of skin cancer typically requires wide excision, a method that creates large defects in the eyelid region [10]. Defects of the facial skin and soft tissue are related to the physiological and anatomical functions of the sensory organs, and as such, appropriate coverage methods must preserve functionality. Managing skin defects around the lower eyelid requires particular attention due to the possibility of complications such as eyelid malpositioning, epiphora, lid edema, and hypertrophic scarring [3]. Ectropion refers to the exposure of the conjunctiva due to eversion of the eyelid margin. It is the most common eyelid malposition [11] and can seriously impact daily life [12,13]. In patients with this condition, foreign bodies enter and irritate the eye with greater frequency, causing redness, infection, and keratitis; in severe cases, corneal ulceration and infectious keratitis can develop. If ulceration and infection are not treated, corneal perforation or blindness can result [14]. To address defects in this region, multiple surgical coverage methods exist, with more in development. The aim of these techniques is to preserve a natural aesthetic appearance and to minimize scarring, while maintaining the eyelidŌĆÖs complex anatomy and function [3,4,10,15].
The use of a sickle-shaped flap to cover lower eyelid defects has several advantages over more traditional approaches. When a local flap is used instead of primary closure, an additional scar from the flap elevation inevitably remains. Since the long axis of the sickle-shaped flap runs parallel to the RSTLs, this additional scar is formed more naturally and has better cosmetic results. In addition, the tension is lower, decreasing the risk of eyelid malposition complications. A final benefit is that this method is very simple and can therefore be easily and quickly completed, even under local anesthesia.
In this study, lower eyelid region defects were analyzed in nine patients who underwent sickle-shaped local flap reconstruction oriented along the RSTLs. All nine sickle-shaped local flaps were taken well without acute complications such as necrosis, and no instances of ectropion or epiphora were encountered during the follow-up period.
The sickle-shaped flap has some disadvantages. First, the scars resulting from the use of such flaps are longer than those associated with Limberg or Dufourmentel flaps used to cover similar-sized defects. However, a shorter scar is not always cosmetically preferable. Elevating flaps in a direction that is inconsistent with the RSTLs may result in shorter scars, but these scars will likely be more prominent (Fig. 5). Sickle-shaped flaps may yield longer scars, but because the scars run parallel to the RSTLs, they remain pliable and flat, with a color similar to that of normal skin. In some cases, therefore, the aesthetic results are better with the sickle-shaped flap.
Another disadvantage is the difficulty in applying this technique across all areas. In addition to the RSTL-defect relationship, it is necessary to consider the location of surrounding landmark structures, which can complicate the application of this technique. Also, it may be difficult to employ sickle-shaped flaps in the repair of circular defects. In such cases, with due consideration of the surrounding landmarks and RSTL, one end of the defect can be cut to form an oval shape.
The present study has several limitations. Since this was a retrospective review, we could not control all of the variables that influenced the outcome. The number of cases was small because we limited the included patients based on the defect area (medial canthal area, lower eyelid, and lateral nose). In addition, we did not objectively compare this surgical method to others, and therefore the benefits of this approach could not be accurately quantified.
In the reconstruction of lower eyelid defects, the sickle-shaped transposition flap could be a simple, fast, and aesthetically favorable surgical option.