INTRODUCTION
With the ever-increasing demand for a higher nasal tip in Asian rhinoplasty, numerous surgical techniques have been introduced [1]. Consequently, complications involving the nasal tip are encountered more often [2]. Especially in revision rhinoplasty where the skin envelope covering the nasal tip has been compromised, surgeons are hesitant to retain the previous projection. Therefore, it would be ideal to identify a technique for retaining the previously achieved nasal projection and providing adequate coverage. The authors propose a method for achieving this goal utilizing a dermofat graft.
CASE REPORT
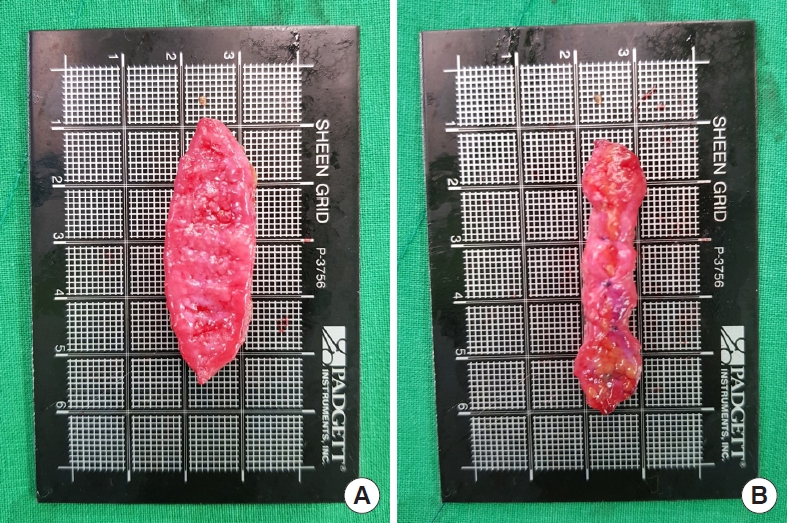
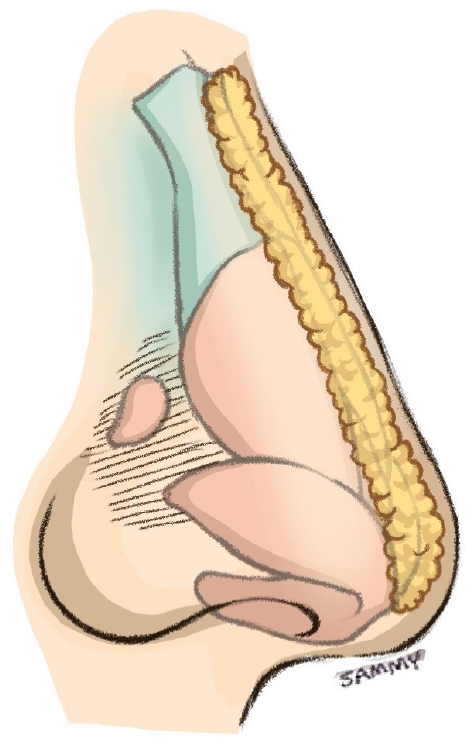
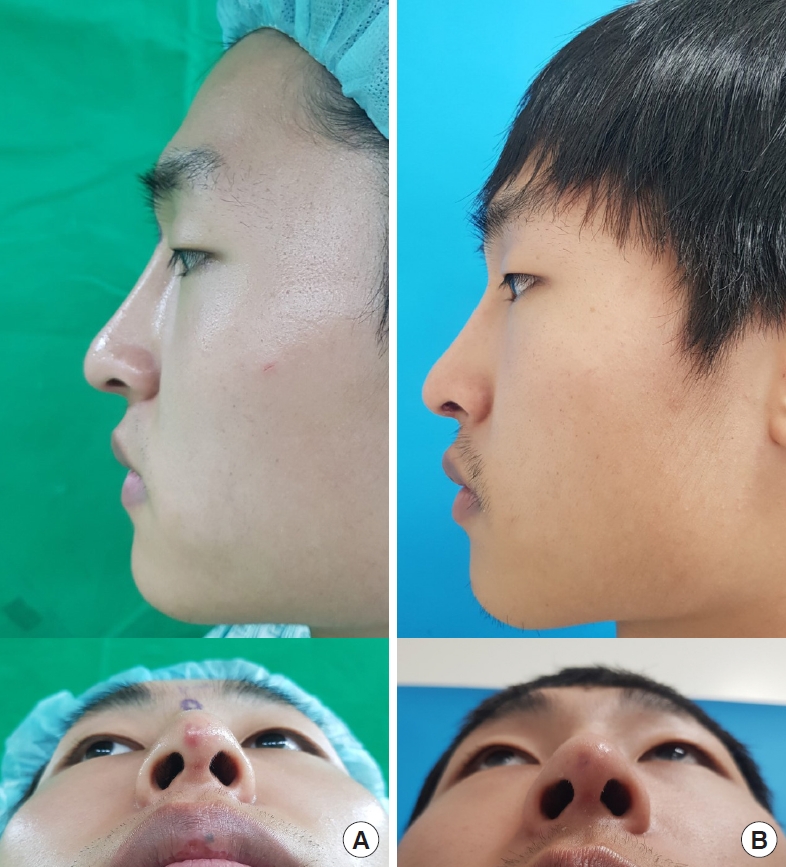
A 23-year-old male patient underwent augmentation rhinoplasty with a septal extension graft and a Gore-Tex implant insertion. After 1 month, the cartilage contour of the nasal tip could be observed through thinned skin due to excessive pressure (Fig. 1). Revision rhinoplasty was planned 2 months after the primary rhinoplasty. The length from the nasal root to tip was measured (5 cm). A dermofat graft was designed in the sacral midline with a longitudinal length that corresponded to the previous measurement. The graft was designed in an elliptical shape (5├Ś2 cm) with an elongation on one end that would later be used for tip coverage (Fig. 2). The extended dermofat graft was designed to provide both replacement of the dorsal implant and sufficient coverage for the nasal tip (Fig. 3). During secondary rhinoplasty, implant removal was performed, and the graft was inserted without modification of the previous tip plasty. The graft was fixed at two points: one point was sutured at the infratip area and the other was fixated with a bolster suture on the nasal root that was removed 5 days postoperatively. Favorable wound healing was achieved (Fig. 4).
DISCUSSION
Rhinoplasty is one of the most frequently performed aesthetic surgical procedures in Asians, in whom the nose has several distinctive features, such as a short columella, flared nostril shape, wide alar base, poorly defined nose tip, and low dorsum [3]. The primary goal of Asian rhinoplasty is to achieve a definite contour by increasing the dorsal height and tip projection [4]. At the same time, the surgical outcomes should be naturally harmonized with other parts of the face.
The thickness of the nasal skin affects both the outcomes and the complication risk after surgery [5]. Anatomically, the nasal skin is thickest in the radix and supratip area and thinnest at the rhinion [6]. However due to excessive tip plasty, skin-related complications after rhinoplasty can be commonly observed in the nasal tip [7]. These complications could cause implant infection and/or extrusion, leading to an irreversible misconfiguration. Although uncommon, managing tip necrosis after rhinoplasty is troublesome [8]. Without adequate skin coverage, tip plasty in rhinoplasty is futile. When revision rhinoplasty is required due to a loss of tip skin integrity, surgeons are forced to reduce the projection.
The increasing popularity of augmentation rhinoplasty has made revision rhinoplasty necessary in increasingly many cases. It is widely acknowledged that secondary rhinoplasty is far more complicated than primary rhinoplasty since only limited surgical options remain. From the perspective of the surgeon, it is a complicated problem to solve, since the desired outcome must be achieved while minimizing the risk of failure. For this reason, selection of an ideal material is a prerequisite for revision rhinoplasty.
Dermofat, an autologous dorsal augmentation material, has distinct advantages. First, sufficient quantities can be obtained from anywhere in the body. In addition, the graft can be easily fixated, and its rapid interaction with the surrounding soft tissue makes displacement less likely [9]. Although it is inferior to synthetic implants in terms of its intrinsic strength and long-term volume maintenance, a dermofat graft is still an effective option in situations where synthetic material cannot be used. Numerous studies have reported favorable outcomes of dermofat grafts, which can be an excellent option, especially for secondary rhinoplasty [10,11].
Dermofat grafts are mainly obtained from the sacral area, where thick dermal tissue can be harvested. Traditionally, dermofat grafts are designed in an elliptical shape with a length equal to that from the nasion to the nasal tip. The cranial and caudal ends are fixated over the nasion and nasal tip with the pull-out suture method. In an open approach, the caudal end can be sutured to the soft tissue of the nasal tip [12]. We have designated our method an ŌĆ£extendedŌĆØ dermofat graft because it has an elongated tail that covers the entire nasal tip up to the infratip area. Thus, it can be performed without modifying the previous tip plasty. As a result, the extended dermofat graft can provide both a replacement for a dorsal implant and soft tissue coverage in the nasal tip, while retaining its previous height. The extended dermofat graft is an optimal substitute for secondary rhinoplasty, especially in cases of damage to the tip skin and soft tissue envelope. The relatively short-term follow-up is a limitation of this study.