A split-face study of moisturizer containing Centella asiatica extract after ablative fractional carbon dioxide laser resurfacing
Article information

Abstract
Background
Ablative fractional CO2 laser treatment is popular for improving atrophic acne scars; however, complications after laser treatment are unavoidable. The purpose of this study was to investigate the efficacy and safety of a moisturizer containing Centella asiatica extract when applied after ablative fractional CO2 laser resurfacing.
Methods
A split-face study was conducted between September 2020 and December 2020 on 34 patients (16 females and 18 males) who were treated with ablative fractional CO2 laser resurfacing. After laser treatment, C. asiatica extract was applied to the right side of the face and purified water was applied to the left side. We compared the right and left sides of the face at various time points after laser treatment using an automatic skin analysis device to investigate the degree of moisture and post-inflammatory hyperpigmentation.
Results
No significant difference in the degree of moisture was found between the two sides of the face immediately after laser treatment (P=0.059), but there was a significant difference at 1 and 4 hours after post-laser treatment care (P<0.001). Regarding post-inflammatory hyperpigmentation, there was no significant difference between the two sides of the face before laser treatment (P=0.184), but a significant difference was found at 6 weeks after laser treatment (P<0.001).
Conclusions
Our results show that applying C. asiatica extract is a novel post-laser treatment modality that can provide satisfactory results without complications after ablative fractional CO2 laser resurfacing.
INTRODUCTION
Ablative fractional 10,600 nm CO2 laser resurfacing is a popular method of treating photoaging, skin laxity, and atrophic scars [1-5]. The mechanism of the ablative fractional CO2 laser is fractional photothermolysis with an ablative 10,600 nm wavelength. It delivers microthermal zones, which are microscopic columns of thermal injury, to a specific fraction of epidermal and dermal tissue [6,7]. The microthermal zones are surrounded by healthy, intact skin, and rapid reepithelization occurs via the migration of cells from the adjacent epidermis and follicular units [1,6,7]. This rapid reepithelization leads to decreased recovery time, side effects, and complications compared to traditional non-fractional laser resurfacing, but recovery time and downtime following ablative fractional CO2 laser resurfacing are often unavoidable [8,9]. Moreover, post-inflammatory hyperpigmentation (PIH) commonly occurs in Asian patients [8,10].
Numerous methods have been introduced to shorten the downtime and the incidence of PIH, such as early sun protection, topical or systemic steroids, and moisturizers with anti-inflammatory agents [3,11]. However, some studies have reported that the application of post-treatment topical steroids could have unfavorable effects on wound healing and increase the incidence of skin infection and acneiform eruption [10,12,13]. Centella asiatica has been used in folk medicine for hundreds of years, and it is traditionally used to improve the condition of small wounds [14,15]. It is also a well-known anti-inflammatory and moisturizing agent [14,15].
The aim of our study, therefore, was to evaluate the efficacy and safety of a moisturizer containing C. asiatica extract when applied after ablative fractional CO2 laser resurfacing.
METHODS
A split-face study was conducted to evaluate the efficacy and safety of a moisturizer containing C. asiatica extract after ablative fractional CO2 laser resurfacing. Of the patients who underwent ablative fractional CO2 laser resurfacing to treat atrophic acne scars between September 2020 and December 2020, 34 (Fitzpatrick skin type IIIIV) who understood and agreed to the purpose and methods of this study were enrolled. Exclusion criteria included keloid scarring, recent use of oral retinoids, pregnancy, immunosuppressive drug use, active systemic or local infections, local skin disease that might alter wound healing, and a history of psychiatric illness.
The study conformed to the principles of the Declaration of Helsinki, and written consent was obtained from each patient for both the surgery and the publication of photographs of the results. The study was approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital (IRB No. 2021-02-016).
Laser treatment
Before laser treatment, topical anesthetic cream containing 2.5% (w/v) lidocaine hydrochloric acid and 2.5% (w/v) prilocaine (a eutectic mixture of local anesthetics cream; AstraZeneca AB, Södertälje, Sweden) was applied under occlusion for 45 minutes prior to laser treatment. All patients were treated using a 10,600-nm ablative CO2 fractional laser (UltraPulse; Lumenis Ltd., Yokneam, Israel) with a size of 10×10 mm (with a 5% overlap) delivered at a fluence of 10.0 mJ/cm2 in 1.00-ms pulses at 300 Hz in the Deep FX mode. All laser safety precautions were followed. After treatment, patients were instructed to clean their faces with mild soap and water daily and to apply full-spectrum sunscreen liberally until the end of the study.
Post-laser treatment care
Each side of the face was treated using different post-treatment methods. A moisturizer containing C. asiatica extract (Kineff 3 Derma Cica Ampoule; Holians Corp., Seoul, Korea) was applied to the right side of the face, and purified water was applied to the left side. Individual sterile cotton buds were used to apply the agents to each side of the face to prevent contamination. After the two agents were applied, a moisture mask (Kineff Hydracica Calming Mask; Holians Corp.) was applied for 30 minutes. The patients were instructed to apply C. asiatica extract (Kineff 3 Derma Cica Ampoule) to the right side of the face and purified water to the left side until removal of the skin crust.
Outcome evaluation
We evaluated the degree of moisture on the face using an automatic skin analysis device (Mark-Vu; PSI Plus Co., Suwon, Korea) immediately after laser treatment (T0), at post-laser treatment care (T1), 1 hour after exposure to room temperature and moisture after post-laser treatment care (T2), and 4 hours after post-laser treatment care (T3). To evaluate PIH, we used an automatic skin analysis system with ultraviolet light at pretreatment and 6 weeks after treatment.
Statistical analysis
Statistical analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA). The Wilcoxon signed-rank test was used to compare the degree of moisture at T0, T1, T2, and T3 and the degree of PIH at pretreatment and 6 weeks after treatment. Statistical significance was set at P<0.05.
RESULTS
Of the 34 patients with atrophic acne scars who were treated using ablative fractional CO2 laser resurfacing, 16 were female and 18 were male. The mean age of the patients was 32.4 years (range, 24–43 years), and the mean follow-up period was 7 weeks (range, 6–8 weeks) (Table 1). The most frequent complications were erythema, edema, and pain, but infection was not observed during the follow-up period.
Demographic characteristics of patients
Using a split-face study, we analyzed the differences in the degree of moisture at various time points after laser treatment. The degree of moisture on the right side of the face was 33 (interquartile range [IQR], 32–35) and that on the left side was 33 (IQR, 32–34) at T0; this difference was not significant. However, the degree of moisture on the right and left sides was 57 (IQR, 56–58) and 52 (IQR, 51–53) at T1, 47 (IQR, 46–48) and 41 (IQR, 40–41) at T2, and 41 (IQR, 40–42) and 34 (IQR, 33–35) at T3, respectively; these differences were significant (P<0.001) (Fig. 1).
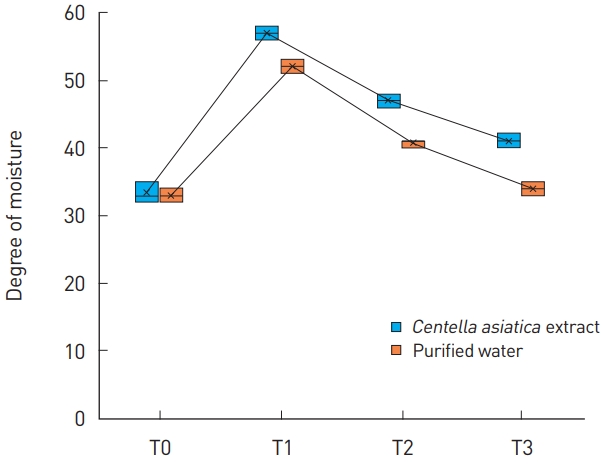
The degree of moisture was investigated at various time points after ablative fractional CO2 laser treatment. There was no significant difference between the right side of the face (to which Centella asiatica extract was applied) and the left side of the face (to which purified water was applied) immediately post-laser treatment (T0) (P=0.059). There was a significant difference between the right and left sides at post-laser treatment care (T1) and 1 (T2) and 4 hours (T3) after post-laser treatment care (P<0.001).
In addition, we evaluated the difference in PIH between the right and left sides of the face. Pretreatment, the degree of PIH was 24.5 on the right side of the face (IQR, 24–25) and 25 on the left side (IQR, 24–25), and the difference was not significant. However, the degree of PIH was 25 on the right side of the face (IQR, 24–25) and 27 on the left side (IQR, 25–28) at 6 weeks after laser treatment, which was a significant difference (P<0.001) (Figs. 2-4).
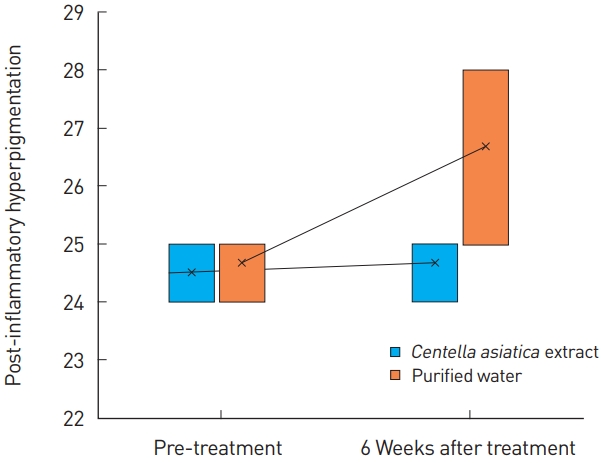
Post-inflammatory hyperpigmentation was investigated at various time points after ablative fractional CO2 laser treatment. There was no significant difference between the right side of the face (to which Centella asiatica extract was applied) and the left side of the face (to which purified water was applied) at pretreatment (P=0.184). A significant difference was found between the right and left sides 6 weeks after treatment (P<0.001).
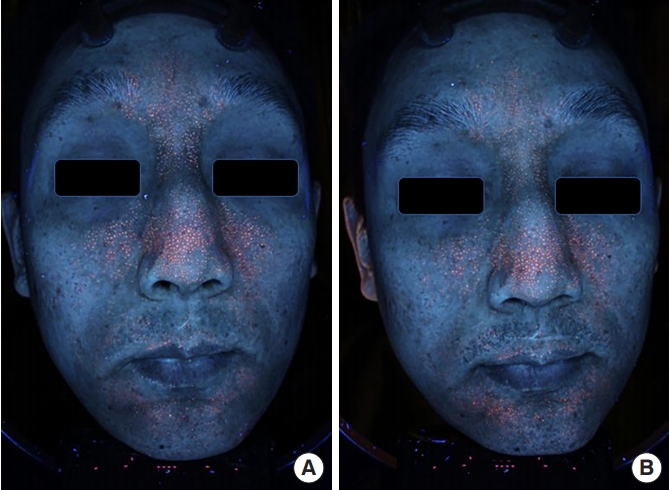
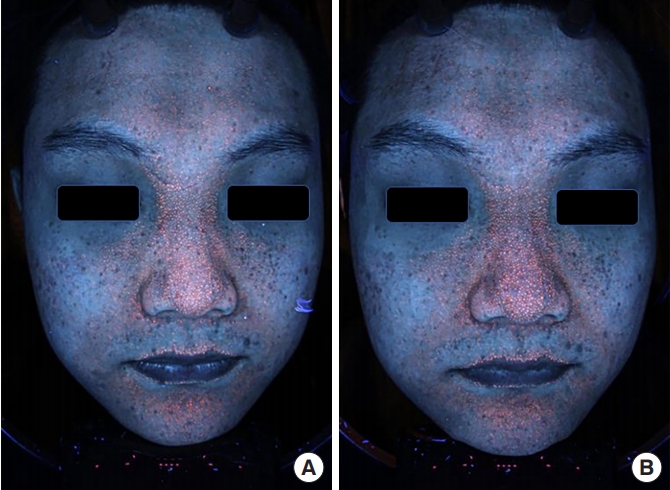
A 28-year-old male patient with atrophic acne scar. We analyzed post-inflammatory hyperpigmentation (PIH) using an automatic skin analysis device (Mark-Vu). At pretreatment, the degree of PIH was 24 on the right side of the face (to which Centella asiatica extract was applied) and 24.5 on the left side of the face (to which purified water was applied) (A). The degree of PIH was 25 for the right side of the face and 26.5 for the left side (B).
A 26-year-old male patient with atrophic acne scar. At pretreatment, the degree of post-inflammatory hyperpigmentation (PIH) was 25 on the right side of the face (to which Centella asiatica extract was applied) and 25 on the left side of the face (to which purified water was applied) (A). The degree of PIH was 25 for the right side of the face and 27 for the left side (B).
DISCUSSION
Although ablative fractional CO2 laser resurfacing can achieve rapid wound healing compared to traditional ablative lasers, it often causes complications associated with wound healing. Wound healing is a complex and dynamic process that can be divided into three phases: inflammation, proliferation, and remodeling [3,16]. In particular, a moist wound environment can provide sufficient and rapid wound healing and avoid post-laser complications, such as infection, hypertrophic scarring, and PIH [8,16].
C. asiatica is a medical plant that has been used for at least 3000 years [14,15]. It contains pentacyclic triterpenes, such as asiaticoside, madecassoside, asiatic acid, and madecassic acid, as its active compounds [14]. Tenni et al. [17] reported a significant increase in the percentage of collagen and fibronectin of a human skin fibroblast after the application of C. asiatica extract. In addition, C. asiatica extract increased collagen synthesis in a dose-dependent manner [18]. C. asiatica extract could facilitate scar maturation by increasing type I collagen synthesis and the type I to type III collagen ratio [19], and it could prevent keloid scar formation by negatively regulating the expression of the transforming growth factor (TGF)-βI and TGF-βII receptor genes and positively regulating the expression of Smad7 [20].
In our study, we evaluated the degree of moisture during postlaser treatment care using a split-face study. The degree of moisture on the right side of the face to which C. asiatica extract was applied post-laser treatment care was higher than that on the left side to which purified water was applied. In addition, we investigated the degree of moisture at 1 and 4 hours after post-laser treatment care; the ride side of the face maintained more moisture than the left side until 4 hours after post-laser treatment care. The differences in moisture between the two sides of the face were significant at postlaser treatment care and at 1 and 4 hours after post-laser treatment care. To investigate PIH, we evaluated the degree of PIH at pretreatment and 6 weeks after treatment using a split-face study. The patients were instructed to apply C. asiatica extract to the right side of the face and purified water to the left side until the skin crusts were removed. At 6 weeks after treatment, the degree of PIH on the right side of the face was significantly lower than that on the left side. Rapid wound healing would provide a moist environment, and rapid wound healing after laser treatment could provide satisfactory results without complications [8,13,16]. Our study results show that applying C. asiatica extract to the face after ablative fractional CO2 laser treatment can provide a moist wound environment and reduce the degree of PIH. Moreover, the results on the effects of C. asiatica extract were obtained using a split-face study to eliminate patient bias.
Therefore, the application of C. asiatica extract could provide a novel post-laser treatment modality to decrease the incidence of PIH and promote rapid wound healing while maintaining a moist wound environment. Nevertheless, further study is recommended because our study has some limitations, including a small sample size, short-term follow-up period, and the inclusion of only an Asian population with Fitzpatrick skin types III-IV.
Although further studies with long-term follow-up periods are needed, in this study, the application of C. asiatica extract provided a moist wound environment to induce rapid wound healing and prevent PIH after ablative fractional CO2 laser resurfacing.
Notes
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital (IRB No. 2021-02-016) and performed in accordance with the principles of the Declaration of Helsinki.
Patient consent
The patients provided written informed consent for the publication and the use of their images.