Dual cortical tunneling method for endoscopic forehead lift
Article information

Abstract
Background
Endoscopic forehead lift with cortical tunneling is an effective option for rejuvenation of the upper third of the face. Although it has been considered safe and reliable, with relatively consistent long-term results, relapse and weakening of adhesion have been common problems.
Methods
We suggest the dual-tunneling method for overcoming these limitations. A total of 100 patients aged 17 to 65 years underwent forehead lifting with cortical tunneling by the senior author from August 2016 to December 2017. The single-tunnel method was applied in one half of the patients and the dual-tunnel method in the other half. Bilateral brow positions were measured immediately following surgery and 6 months later.
Results
For all cases, cortical tunneling was done at the central incision and both paramedian incisions; therefore, three tunnels were used in the control group and six tunnels in the experimental group. In the single-tunnel group, relapse distances were 2.39±0.83 mm for the medial brow and 3.26±0.91 mm for the lateral brow (6 months postoperatively; n=100). The dual-tunnel group showed significantly smaller (P<0.001) relapse distances, with values of 1.69±0.46 mm and 2.17±0.59 mm for the medial and lateral brow, respectively (6 months postoperatively; n=100). The experimental group did not show an increase in complications.
Conclusions
The dual-tunneling method, designed to minimize the cheese-wiring effect, uses a triangular plane to avoid a focal fixation. The fixation also includes the periosteum to hold the forehead tissue in place, inducing stronger adhesion.
INTRODUCTION
For patients with aging problems in the upper third of the face, such as functional brow ptosis, dermatochalasis, and wrinkles of the forehead or glabella, endoscopic forehead lift may be an effective option for rejuvenation [1]. There is a wide choice of fixation methods including skin adhesives, tacks, bolsters, Kirshner wires, cortical tunneling, or screw fixation [2], each with respective advantages and drawbacks. Although there have been no randomized controlled studies regarding the choice of fixation method, there are noteworthy reports in the literature concerning this issue. For instance, Jones and Grover [3] reported that suture fixation via cortical tunneling produced reliable and relatively consistent long-term results compared to fibrin glue fixation. However, relapse and weakening of adhesion are common problems related to the cheese-wiring effect of cortical tunneling, which can be attributed to its reliance on a single-point fixation. In this study, we suggest a dual-tunnel method for overcoming the limitations of conventional calvarial fixation dependent on a single cortical tunnel.
METHODS
All patients who visited the clinic for endoscopic forehead lift were examined and evaluated by the senior author (WT). Preoperatively, all patients were photographed, and designs were marked in the sitting position (Fig. 1).

An example of the preoperative design in a sitting position.
The single-tunnel method was applied for 50 patients and the dual-tunnel method was used for the other 50 patients. The effectiveness of the procedure and relapse rate were evaluated by measuring the position of the brow before surgery, immediately following surgery, and 6 months later. All operations and measuring were done by the senior author.
For each operation, incisions were made at five points: two temporal, two paramedian, and one at the center, as described by Isse [4]. Then each depressor muscle (corrugator, depressor supercilii, procerus, and medial head of the orbicularis oculi) was appropriately avulsed or resected. For all cases, cortical tunneling was done at the central and both paramedian incisions; therefore, three tunnels were used for fixation in the single-tunneling group and six tunnels in the dual-tunneling group. A single tunnel was made in the caudal to cephalic direction, whereas a dual tunnel was designed more obliquely at the same site or posterior to the cephalic hole of a single tunnel (Fig. 2).
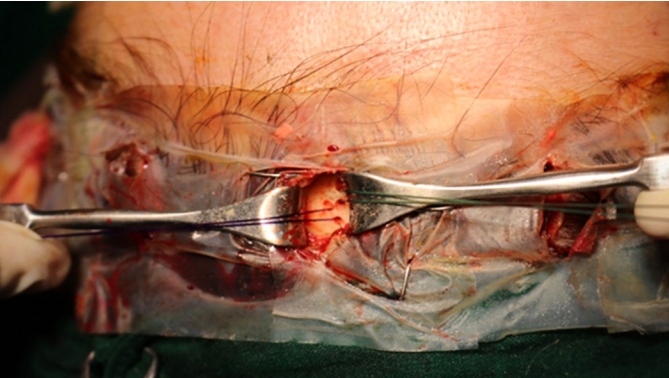
The dual-tunnel method showing caudal and cephalic tunneling. A single tunnel was made in the caudal to cephalic direction, whereas a dual tunnel was designed more obliquely in the same site or more posterior to the cephalic hole of a single tunnel.
All relevant depressor muscles and periorbital ligaments were released according to the preoperative design. A 1.2-mm burr head was used for cortical tunneling. The caudal fixation included tissues at the subcutaneous level to the periosteum in a vertical fashion, while the cephalic fixation anchored the periosteum and galea in a horizontal fashion, allowing further stabilization. The distance between the two tunnels was 3–4 mm. All fixation was done with #2-0 Ethibond (round needle; Ethicon, Somerville, NJ, USA) for the caudal side and #2-0 polydioxanone (round needle) for the cephalic side.
Brow positions were measured serially at the medial side and lateral side of the brows, bilaterally. Each patient was asked to close his or her eyes, and measurements were made to determine the distance from the lower margin of the medial and lateral sides of the brow to the palpebral fissure. Along with brow positions, the lifted distance was recorded and used for a statistical analysis of the effectiveness of the procedure and the degree of relapse. To analyze the results, we used SAS version 9.3 (SAS Institute Inc., Cary, NC, USA) to apply the independent two-sample t-test in a linear mixed model.
RESULTS
A total of 100 patients aged 17 to 65 years underwent forehead lifting by cortical tunneling from August 2016 to December 2017. The mean values of the serial measurements of brow position, including lifted distance, are outlined in Table 1. In the single-tunneling group, the total brow elevation distance was 8.36±1.04 mm and 7.78±1.57 mm for the medial and lateral brows, respectively. The relapse distances were 2.39±0.83 mm for the medial brow and 3.26±0.91 mm for the lateral brow at 6 months (n=100). In the dual-tunneling group, total brow elevation was 7.98±0.84 mm for the medial brow and 7.60±1.24 mm for the lateral brow. The relapse distances at 6 months postoperatively were 1.69±0.46 mm and 2.17±0.59 mm for the medial and lateral brow, respectively (n=100).

Serial measurement of the eyebrow position in terms of the distance between the lower margin of the eyebrow and the upper eyelid
Initially, patients in the single-tunnel group had a larger lateral brow to lower eyelid distance (19.89±2.44 mm) compared to the experimental group (18.93±2.11 mm, P=0.004). The elevated distance at the medial brow was also larger in the single-tunnel group (8.36±1.04 mm) than in the dual-tunnel group (7.98±0.84 mm, P=0.006). Immediate postoperative measurements showed that the single-tunnel group had a larger distance from the medial and lateral brow to lower eyelid (P=0.024 for medial, P<0.001 for lateral). Although no statistically significant difference in the absolute brow position was observed between the two groups at 6 months postoperatively, the dual-tunneling group did show smaller relapse distances (Figs. 3, 4).
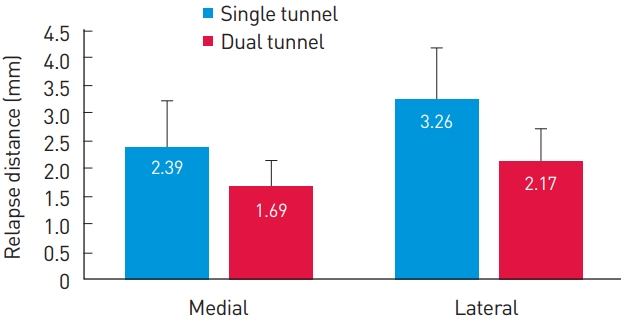
Comparison of relapse distance at 6 months postoperatively between the single-tunnel and dual-tunnel groups. The dual-tunnel group showed a significantly smaller relapse distance at both the medial and lateral portions of the eyebrow (P<0.001).

A preoperative (A) and 6 months postoperative (B) picture of a 62-year-old female patient.
No significant complications such as hematoma, nerve damage, alopecia, or infection were observed during the 6 months of follow-up.
DISCUSSION
After its introduction in the 1990s by Vasconez [5], endoscopic forehead lifting gained popularity for rejuvenation of the upper third of the face, and several fixation techniques for anchoring lifted soft tissue have been introduced [2]. If secure and durable fixation is not ensured, relapse of brow ptosis is a common problem, even after sufficient dissection and release of forehead soft tissue. Since McKinney et al. [6] introduced calvarial fixation of lifted forehead tissue via cortical tunneling, advocates of the method have confirmed its safety and reliability [7]. However, long-term drooping of the eyebrows, especially the lateral portion, has been observed. The dual-tunneling method was designed to minimize drooping of tissues attributable to the cheese-wiring effect observed in the single-tunnel method. This is achieved by avoiding a focal fixation, instead using a triangular plane including the periosteum to secure the forehead tissue in place, thus providing stronger fixation until adhesion occurs and minimizing the gradual tearing of fixated tissue from a single suture. In addition, by distributing pressure at the fixation point, dimpling of tissue is less likely to occur.
This method resembles the principle behind the Endotine fixation device. Honig et al. [8] compared the results of single tunnel cortical tunneling and the Endotine fixation method and showed that Endotine fixation provided a more stable medial brow position than conventional cortical tunnel fixation with sutures. The authors suggested that, by distributing tension over multiple points, Endotine fixation enhances the suspension of lifted tissue. However, even Endotine fixation did not prevent drooping of the lateral brow over time. In our study, even though the overall lifted distance of the lateral brow was not significantly different between the single-tunnel and dual-tunnel groups, the dual-tunnel group had a significantly smaller relapse distance. Although vertical lift of the lateral brow has been less emphasized in Asian patients due to the risk of accentuating a preexisting Mongolian slant [9], this result is meaningful in that fixation via dual tunneling provided superior maintenance of the lifted forehead flap even in the lateral portion of the brow. Strengthening fixation on the temple side will prevent future drooping of the lateral brow.
Additionally, it is notable that while palpability was found in most patients who underwent Endotine fixation [10], no distinct palpability was found in patients when the tunneling method was used. It has also been reported that degradation of the Endotine device requires time and that a foreign body reaction can occur with giant cell aggregation [11], whereas no noteworthy foreign body reaction was found in patients when the tunneling method was used.
For Asian cases in particular, more than two Endotine fixation devices are usually needed due to the emphasis on medial brow elevation. Considering palpability and the cost of surgery using exogenous fixation material such as with the Endotine method [12], dual cortical tunneling fixation may be a reasonable alternative without the need to purchase and implant an exogenous device.
There is no standardized protocol for measuring the height or position of an eyebrow. Although a common method is measuring the distance between mid-pupil and the lower margin of the brow with the patient gazing straight ahead in a sitting position [13], we chose to measure the distance between the palpebral fissure and the lower margin of the brow with the patient’s eyes closed. In this way, we tried to minimize any voluntary or involuntary compensatory movement of the frontalis muscle that could confound the measurements. This principle was discussed and applied by Jung et al. [14], in their study of the eyebrow position and shape preferred by Korean women. They measured the height-to-width ratio when eyes were closed to evaluate the change in eyebrow shape and position with age. Using measurements done while subjects closed their eyes, Jung et al. showed that the height-to-width ratio decreased with age, in contrast to previous studies where measurements were usually done with the eyes open. Even when patients were asked to open their eyes and relax the frontalis muscle, it was hard to eliminate involuntary movements. Additionally, some patients with eyelid ptosis tilt their head backward when gazing straight ahead, making accurate measurements even harder. By asking patients to close their eyes, we tried to minimize these confounding factors.
Of note, slightly longer incisions and additional operation time are needed for dual tunneling. Incisions are lengthened by two to three millimeters and the operation takes 5 to 15 minutes longer compared to the single-tunnel method. However, no incision site complications such as alopecia or unacceptable scarring (e.g., depressed scar) were observed. Also, some surgeons might prefer to use an Endotine device since cortical tunneling has a considerable learning curve compared to the Endotine technique.
Appropriate management of brow depressor muscles and the release of periorbital ligaments are prerequisites, regardless of which type of fixation a surgeon decides to employ. Only after proper endoscopic manipulation of the relevant musculature and ligaments is a comparison of different fixation methods relevant. In addition, the handling of the brow depressor muscle is especially important in Asian patients to achieve satisfactory results in elevation of the medial brow.
Notes
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Institutional Review Board of Severance Hospital (IRB No. 2022-1930-001) and performed in accordance with the principles of the Declaration of Helsinki.
Patient consent
The patients provided written informed consent for the publication and the use of their images.