INTRODUCTION
Aesthetic or reconstructive surgical procedures using breast implants are routinely performed, and in increasing numbers [1]. Capsular contracture is the most common complication after breast implant surgery, with reported incidence rates ranging from 2.8% to 20.4% [2,3]. Capsular contracture is caused by an excessive fibrotic reaction in the tissue surrounding the implant and is thought to be an inflammatory response [2]. The precise etiology and pathogenesis of capsular contracture remain unclear, although smooth implants and subglandular position are risk factors [4,5]. Capsular contracture can lead to deformed or painful breasts. In symptomatic capsular contracture (Baker grade III and IV), surgical treatment is needed. Capsulectomy with or without capsulotomy is routinely performed [4]. However, the rate of contracture recurrence after surgical treatment has been found to be 25%, with most cases occurring within 5 years [6]. Therefore, various procedures have been performed to prevent recurrence. Autologous fat transfer and the use of acellular dermal matrix have been reported for the treatment of capsular contracture [7,8]. We present a novel and effective treatment using serial fat grafting before augmentation with implants.
METHODS
Our treatment was performed in patients diagnosed with severe capsular contracture (Baker grade III and IV). Under general anesthesia, the breast implants were removed via an inframammary fold incision. Partial capsulectomy was then performed. The anterior capsule was completely removed, and open capsulotomy was performed with multiple incisions at the posterior capsule. After copious irrigation with antibiotic solution (500 mL of saline, mixed with 1 g of cefazolin and 80 mg of gentamicin), the incision site was closed layer by layer after drain insertion. Fat was harvested from the flank or thigh with a conventional liposuction cannula measuring 3 mm in diameter, under low pressure. The harvested fat was centrifuged at 3,000 rpm for 3 minutes. The purified fat was grafted through the periareolar and axillary incision sites with a 17-gauge cannula measuring 15 to 23 cm in length. Fat was grafted in small aliquots in the subdermal, subcutaneous, and subglandular planes to prevent fat necrosis. The injection plane, injection site, and fat volume were determined by the thickness and circulation status of the breast envelope. The remaining fat was frozen for storage at −20°C. Following fat grafting, a mild compressive dressing was performed using a cotton roll and elastic bandage. One month after the first operation, a second fat graft was performed with the stored fat using the same surgical procedure. One month later, the third fat graft was performed. Six months after the first operation, breast augmentation with implants was performed via the previous inframammary incisions, along the same plane of insertion.
RESULTS
With the progression of fat grafting, we observed thickening and softening of the breast envelope. The irregular surface after capsulectomy and breast asymmetry was corrected through serial fat grafting. No scarring or fibrosis of the breast envelope after capsulectomy was detected. No other significant complications were found. The volume and contour of the breasts were satisfactory to the surgeons and the patients alike.
Case
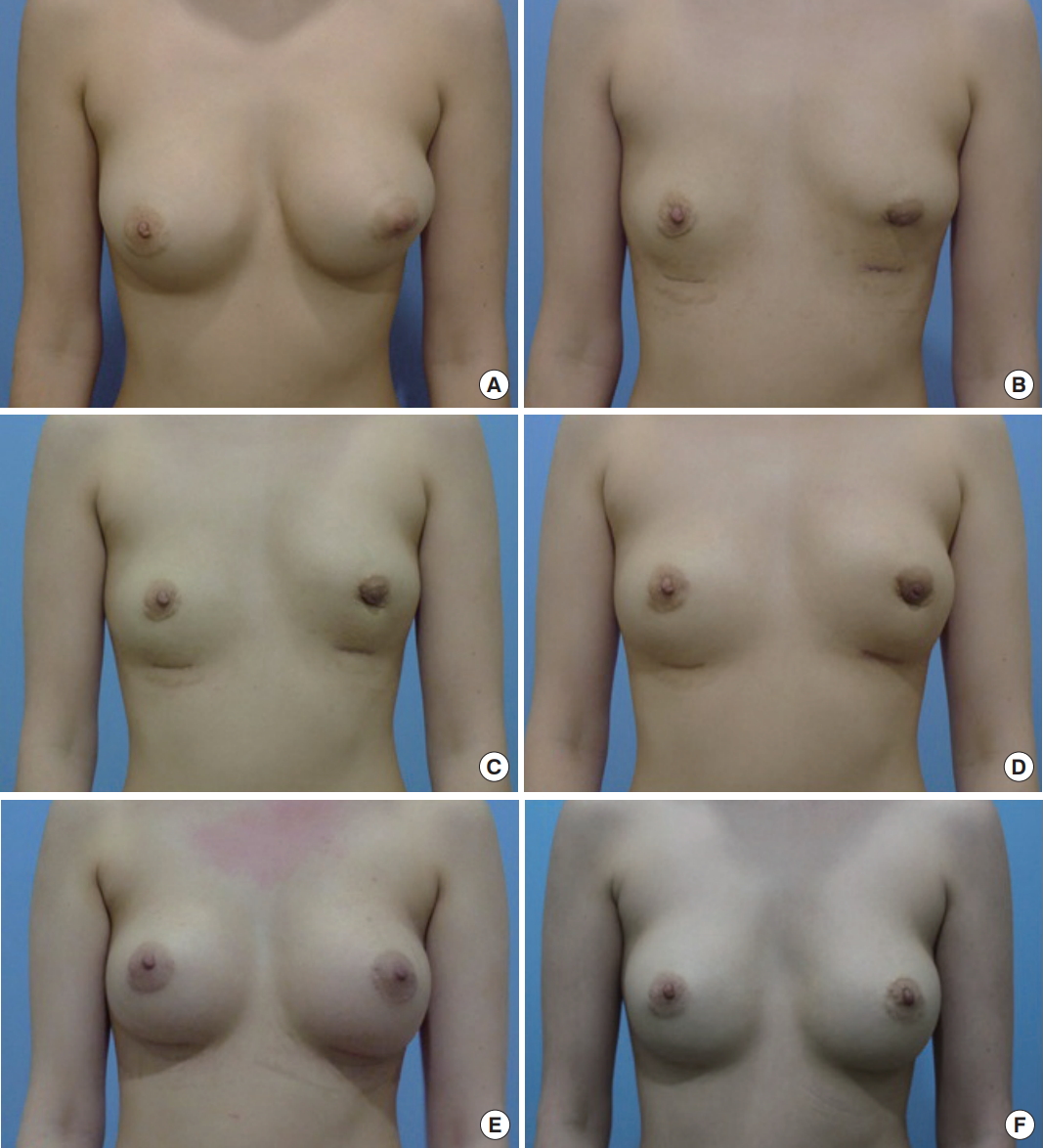
A 33-year-old woman with capsular contracture classified as Baker grade III (right) and grade IV (left) presented with a history of augmentation mammoplasty through a periareolar incision with round textured breast implants (right, 280 mL; left, 240 mL) performed 5 years ago. After implant removal, 69 mL (right) and 84 mL (right) of fat was initially grafted. A month later, a second fat graft with 45 mL (right) and 78 mL (left) of fat was performed. After another month, a third graft was performed using 48 mL (right) and 72 mL (left) of fat. Six months after implant removal, the breasts were augmented with round textured breast implants (right, 220 mL; left, 220 mL) through an inframammary incision. During the follow-up period, which extended for almost 19 months postoperatively, no recurrence of capsular contracture was observed, resulting in a satisfactory aesthetic outcome (Fig. 1).
DISCUSSION
In 1912, Holländer [9] first described fat injection into the breast. However, in 1987, the American Society of Plastic Surgeon (ASPS) condemned the procedure because of concerns that it could interfere with the diagnosis of breast cancer [10]. Nonetheless, fat grafts into the breast have been performed in clinical settings. Coleman and Saboeiro [11] reported positive outcomes of fat grafting into the breast. Recently, several studies reported that fat grafting did not interfere with mammographic interpretation [12,13]. The ASPS stated in 2009 that “fat grafting may be considered for breast augmentation and correction of defects associated with medical conditions and previous breast surgeries; however, results are dependent on the technique and surgical expertise” [10]. Its clinical indications include breast augmentation, reconstruction after breast cancer surgery or radiotherapy-induced breast tissue damage, and the correction of breast deformities [10]. In addition, fat grafting is indicated for the treatment of capsular contracture, as well as breast augmentation with or without implants. A recent porcine model suggested that fat grafting may be used to treat capsular contracture by promoting neovascularization in the adjacent tissue and softening of the capsule [7]. Consistent with our method, Salgarello et al. [14] reported that fat grafting in irradiated breast tissue before implantation reduced radiation-related complications. Panettiere et al. [15] reported that serial fat grafting improved the outcomes of irradiated breasts that were reconstructed with implants. In one case, Baker grade III and IV contracture was downgraded to Baker grade I contracture after a single fat graft.
These therapeutic effects of fat grafting have been attributed to the regenerative effect of adipose-derived stem cells contained in the fat tissue. Adipose-derived stem cells secrete various cytokines, including angiogenic factors, which induce angiogenesis and wound healing [7,14,15].
Our findings suggest that thinning and fibrotic changes after capsulectomy were altered by the treatment. Serial fat grafting thickened and softened the breast envelope. Fat grafting itself augmented breasts, suggesting that smaller breast implants could be used. Therefore, our method prevented thinning of the breast envelope and recurrence of capsular contracture following breast augmentation using implants. In addition, fat grafting corrected surface irregularities and breast asymmetry after capsulectomy. The grafting procedure was conducted 3 times at 1-month intervals due to the limited space available following fibrosis after capsulectomy. A large volume of fat may increase the risk of necrosis due to poor vascularization. Further, the varying conditions of the breast envelope in patients require evaluation at monthly intervals in order to ensure the safety and effectiveness of the serial interventions.
Nonetheless, when using frozen stored fat, it is important to consider the possibility of reduced viability and infection resulting from the freezing and thawing process.
Our results show that serial fat grafting before augmentation with implants in cases of severe capsular contracture resulted in satisfactory functional and aesthetic outcomes, without implant-related complications. Our method represents an attractive treatment modality for cases of capsular contracture.