INTRODUCTION
Postoperative temporal hollowing can occur after craniectomy or cranioplasty for intracranial hemorrhage [1,2]. This complication can be caused by the disinsertion or displacement of the temporalis muscle and atrophy of the superficial temporal fat pad [3]. Postoperative temporal hollowing is generally known to occur within 6 months of surgery and can be a cosmetic problem because it creates an asymmetric facial contour [4].
The classic procedures used to correct temporal hollowing deformities include autologous bone grafts and fat grafts. Alloplastic implants such as polyetheretherketone or porous polyethylene implants have also been used for reconstruction [5,6], as well as custom-made silicone implants. Each method has advantages and disadvantages [7].
Reflecting the increasing interest in rapid, minimally invasive aesthetic procedures, we introduce a case of postoperative temporal hollowing correction using a polydioxanone (PDO) thread-lifting (typically used in facial rejuvenation procedures) along with a simple fat graft.
CASE REPORT
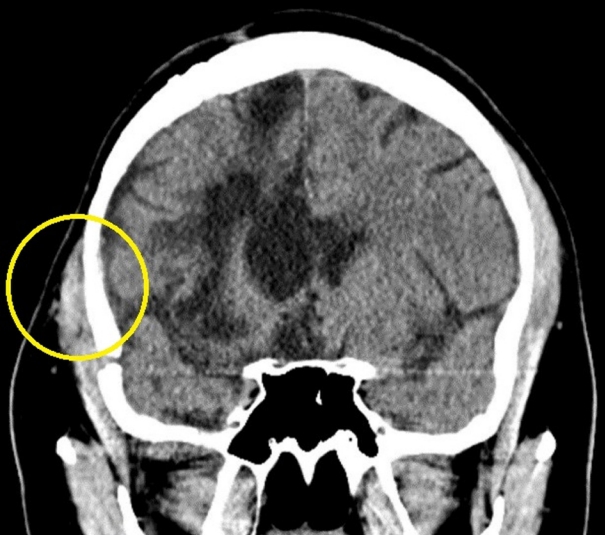
A 28-year-old male patient underwent a craniotomy at the department of neurosurgery after a traffic accident on December 12, 2020. Two months later, a cranioplasty using stored autologous bone was performed. Approximately 6 months after the cranioplasty, the patient presented in the department of plastic and reconstructive surgery for cosmetic correction of right temporal hollowing and asymmetric bulging in the right zygomatic region. The patient did not want a permanent foreign body or implant inserted. He wanted a simple and effective procedure with a short recovery period so that he could quickly return to social activities. Preoperative computed tomography identified partial disinsertion and atrophy of the temporalis muscle (Fig. 1).
Primary fat graft
Using a two-stage procedure, we first performed an autologous fat graft to partially correct the hollowing of the right temporal region. The abdomen was used as the donor site, and the grafted fat was centrifuged at 3,000 rpm for 2 minutes for purification. This resulted in a total of 21 mL of fat, of which 7 mL was injected and the rest stored at –20 °C in a tissue storage freezer. The fat was transplanted into the subcutaneous layer in a radial fashion using a Coleman infiltration cannula through two entry points on the hairline and scalp.
Secondary fat graft and thread-lifting
A month after the first procedure, the second procedure was performed. Under local anesthesia, 4 mL of stored centrifuged fat was injected in the same way as in the previous procedure. After the fat graft, a thread-lift was executed using four threads (Mint Lift; HansBioMed Corp.). One entry point in the right temporal area was used. The incision was made with a #11 scalpel blade, and careful dissection was done with small Metzenbaum scissors to identify the deep temporal fascia. The threads were then inserted into the fascia in the bulging zygomatic region, pulled toward the entry point, and tied (Fig. 2).
No complications occurred during the 4-month follow-up, and the patient was satisfied with the cosmetic results.
DISCUSSION
Postoperative temporal hollowing is a depression in the temporal region that can occur after cranial surgery. It is the result of atrophy of the superficial temporal fat pad (caused by ischemia or denervation) and disinsertion or atrophy of the temporalis muscle [1].
Various methods are used to reconstruct temporal hollowing with alloplastic materials, such as poly-methyl-methacrylate, hydroxyapatite, and polyetheretherketone [7]. This type of correction can be performed without donor site morbidity. However, the size of the incision to allow implant insertion can be large, dissection is necessary, and disadvantages such as infection, breakage, and thermal damage have been reported [8]. Another traditional method of reconstruction uses autologous tissue (e.g., bone grafts, dermofat grafts, and fat grafts). However, donor site morbidity, inadequate engraftment, and limitations of the volume of harvested tissue can be problematic [7]. Because reconstruction for temporal hollowing is performed near scar tissue from a previous operation, the survival rate of the autologous graft can be affected by a hostile tissue environment [9]. However, fat grafting is a commonly chosen surgical method due to its various advantages and technical convenience, whether as a main procedure or an auxiliary procedure [9,10]. Reconstruction using autologous fat grafts is reported to be an effective and safe procedure for treating scars of different origins and is capable of achieving architectural remodeling with loose connective tissue regeneration [11]. The initial fat graft volume remains relatively stable and can easily be increased as necessary. Autologous grafts have a safety advantage because there is no graft rejection or hypersensitivity reaction [9]. Based on these advantages, autologous fat grafting was performed in our case. Although results vary, in our case supplementary grafting was performed 1 month later because the volume of grafted fat had been partially absorbed over time. In addition, the volume of the atrophied superficial temporal fat pad was anatomically increased using a fat graft. Thread-lifting, which is widely used for aesthetic purposes, was applied to manage the bulging in the zygomatic area, which in this case was caused by sagging due to atrophy of the temporalis muscle. Thread-lifting is a minimally invasive technique used to improve the contour of soft tissue [7,12]. The thread (Mint Lift; HansBioMed Corp.) used for thread-lifting in our case has a barbed surface and consists of PDO [13]. After contact with the tissue, the barb applies tensile strength and maintains the arrangement of the moved tissue when pulled [13,14]. Unlike nonabsorbable threads such as nylon, PDO interacts with myofibroblasts in the metabolism of the thread and forms a homogeneous fibrous capsule in the tissue near the thread. This fibrous capsule helps maintain the traction force, which lasts 4 months to 2 years [13,15]. The thread used in our case was an 18-gauge cannulated thread with a length of 170 mm per line and a diameter of 0.49 mm (1-0 size). The procedure is safe because the thread is inserted with a blunt cannula, the procedure time and recovery period are relatively short, and the effect duration time is guaranteed (as described above). In our case, to insert a thread into the fascial layer and to target the zygomatic region with the greatest degree of bulging as much as possible, the fascia was identified after the incision and the thread was inserted along the fascial layer. When performing thread lifting for cosmetic purposes, the thread is inserted targeting the facial superficial musculoaponeurotic system layer as well as the subcutaneous layer to increase the chances for a lasting effect [13]. Considering stability and safety in each procedure, fat grafting was performed first, followed by thread-lifting. The anchoring of the thread-lifted tissue was well maintained, and the volume of the grafted fat was well preserved during the 4-month follow-up period (Fig. 3).
In this case, postoperative temporal hollowing was effectively improved through a combination of autologous fat grafting and PDO thread-lifting, a simple and safe procedure. Although the full effect of this method may not be permanent, there are many advantages in terms of duration and effectiveness. This method is a recommended option for the reconstruction of temporal hollowing, especially for patients seeking a quick recovery and satisfaction with the cosmetic results.