Preseptal upper eyelid lipoma: a case report
Article information

Abstract
Lipomas are benign soft-tissue tumors that typically progress gradually. In this case report, we describe a 77-year-old woman who presented with a mass on the left upper eyelid. An ophthalmologic examination was normal, and ultrasonography revealed a 1-cm ill-defined mass in the subcutaneous fat layer of the left upper eyelid. The tumor was completely excised surgically, and a histopathological examination showed mature fibro-adipose tissue consistent with a lipoma. The patient had an excellent postoperative prognosis. Even though eyelid lipomas are extremely rare, it is important to carefully examine the integrity of the orbital muscle, orbital septum, and levator aponeurosis. Lipoma should be distinguished from herniated orbital fat or the lacrimal glands in the differential diagnosis of an upper eyelid mass.
INTRODUCTION
Lipomas are benign soft-tissue tumors that typically progress gradually. Histologically, they are distinguished by adipose cells, which may be enveloped in a thin fibrotic capsule. Lipomas typically develop in the subcutaneous layers of the back, posterior neck, and extremities [1]. Few cases of eyelid lipomas have been reported in the literature. Some variants of eyelid lipomas have been discussed, including myolipoma [2], intramuscular lipoma [3], angiolipoma [4], osteolipoma [5], pleomorphic lipoma [6], spindle cell lipoma [7], and dermolipoma [8]. However, simple lipomas of the upper eyelid affecting only the preseptal area are very rare, to the best of our knowledge [9]. Herein, we present a case of simple lipoma of the preseptal upper eyelid.
CASE REPORT
A 77-year-old woman presented with a lump on the left upper eyelid that had been there for a year. She experienced no pain or symptoms other than minimal irritation as the mass gradually grew (Fig. 1). The patient reported no history of surgery, injectable cosmetic fillers, infection, inflammation, or trauma to the affected eyelid. The ophthalmologic examination was otherwise unremarkable. Upon examination, there was a soft and rubbery mass measuring approximately 1.5 cm on the left upper eyelid. Ultrasonography was then performed. A 1-cm, ill-defined isoechoic to hyperechoic mass in the left upper eyelid with suspicious internal linear striation was detected (Fig. 2). Based on these findings, a soft-tissue tumor was the most strongly suspected diagnostic possibility.
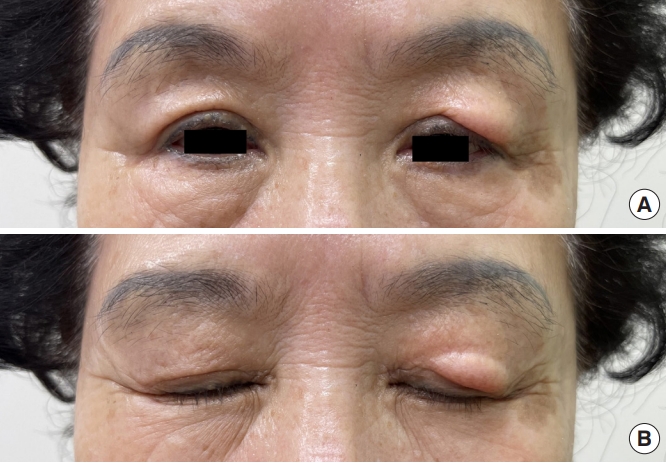
A preoperative photograph of the patient demonstrating bulging of the left upper eyelid.
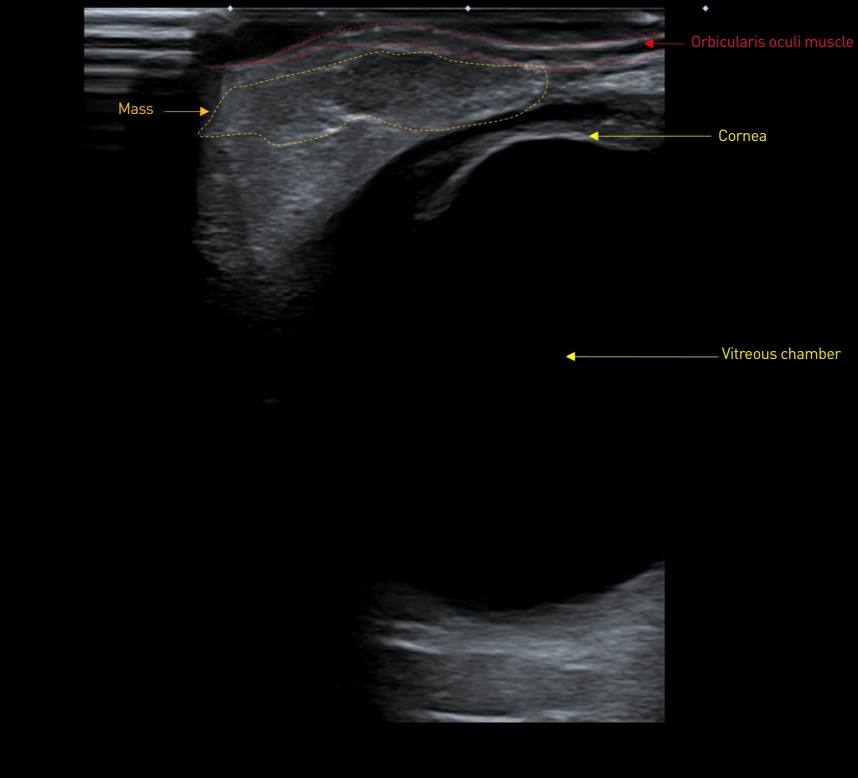
An ultrasonographic image demonstrating a 1-cm, ill-defined, isoechoic to hyperechoic mass in the left upper eyelid, with suspicious internal linear striation.
The patient decided to undergo an excisional biopsy under local anesthesia. An incision was made in a natural supratarsal skin crease, and the orbicularis oculi muscle was divided in the direction of the muscle. Encapsulated multinodular fat tissue was exposed immediately behind the orbicularis oculi muscle, adhering to the orbital septum, levator aponeurosis, and orbicularis oculi muscle (Fig. 3). The orbital septum remained intact without perforation. Additionally, there was no association between the orbital fat and the conjunctiva. Total gross removal was carried out. Microscopically, the tumor was partly encapsulated by thin fibrous tissue and composed of mature fat cells with no cellular atypia. The tumor cells were relatively uniform in size and shape (Fig. 4). The findings were consistent with simple lipoma. No functional deficits or postoperative complications were observed. After 10 months of follow-up, no sequelae or recurrence was observed (Fig. 5, Supplementary Video 1).

An intraoperative photograph of the eyelid crease incision. The sub-orbicularis oculi muscle and preseptal area were found to have multinodular adipose tissue.
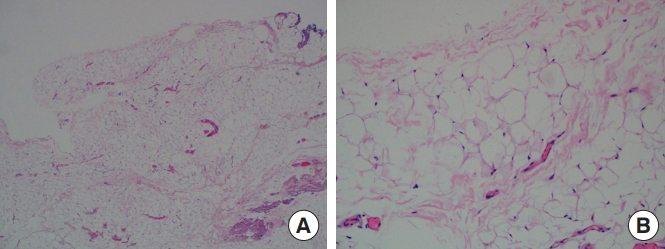
A histopathology photograph. (A) The tumor is partly encapsulated by thin fibrous tissue and composed of mature fat cells (hematoxylin and eosin stain, ×2.5). (B) The tumor cells are relatively uniform in size and shape with no cellular atypia (hematoxylin and eosin stain, ×40).
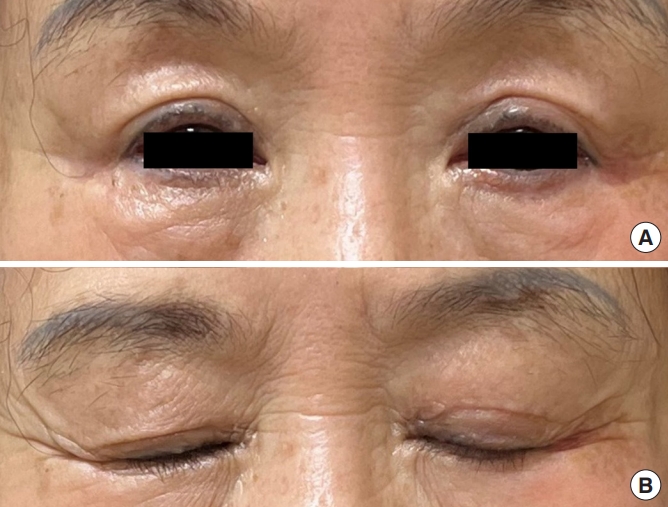
A 10-month follow-up postoperative photograph of the patient with no functional deficits.
DISCUSSION
The eyelids are composed of an anterior lamella, formed of skin; subcutaneous tissue, including its adnexa and orbicularis oculi muscle; and a posterior lamella, formed by the tarsus with the meibomian glands and the palpebral conjunctiva [10]. Similar to tumors of other organs, eyelid tumors can be categorized according to their origin and malignancy. The majority of eyelid tumors are benign and epidermal in origin, whereas adnexal and stromal tumors are less frequent [11]. A few cases of eyelid lipomas have been reported in the literature; however, simple lipomas of the eyelid affecting only the preseptal area are extremely rare [9]. From this point of view, our reported case is distinctive in terms of the origin and location of the tumor.
In previously documented cases of upper eyelid lipoma, the main clinical characteristics were progressive drooping of the upper eyelids, upper eyelid edema, and a palpable mass that became larger while exhibiting no signs of inflammation, such as pain, redness, or skin abnormalities [5,9]. In our case, there was a palpable lump along with the typical clinical symptoms of dermatochalasis. This case, which occurred in an elderly patient and did not involve symptoms, could easily have been misdiagnosed as lateral hooding resulting from dermatochalasis or a herniated lacrimal gland. Since it is important to distinguish those conditions from benign lipomas in elderly patients, the author believes that this case is meaningfully different from the previous literature and is of educational value.
Simple lipomas of the upper eyelid are treated surgically, and the procedure is typically relatively uncomplicated. However, the anatomy of the upper eyelids is complex, and changing one structure may have implications for all its anatomic components. The upper eyelid region represents a surgically challenging site. Therefore, a successful surgical procedure depends on preserving the essential function of the eyelid and achieving proper symmetry with aesthetic proportions [12]. For this reason, when performing surgical excision of a lipoma of the upper eyelid, the integrity of the orbital septum, levator aponeurosis, and orbicularis oculi muscle should be thoroughly inspected and distinguished from herniated orbital fat or the lacrimal gland [13]. In our case, we confirmed that the lipoma adhered to the orbital septum, levator aponeurosis, and orbicularis oculi muscle. However, there was no connection with the orbital fat or conjunctiva. After the excision was completed, there were no impairments of structural integrity or functional deficits at the postoperative follow-up.
Despite the rarity of eyelid lipomas, they should be considered in the differential diagnosis of upper eyelid masses. Ophthalmic and ultrasound examinations should be performed to obtain a precise preoperative diagnosis. Furthermore, when performing surgery, the integrity of the orbital muscle, orbital septum, and the levator aponeurosis must be carefully examined and distinguished from herniated orbital fat or the lacrimal gland, especially in elderly patients.
Notes
No potential conflict of interest relevant to this article was reported.
Ethical approval
The report was approved by the Institutional Review Board of Soonchunhyang University Hospital (IRB No. 2022-10-015).
Patient consent
The patient provided written informed consent for the publication and the use of her images.
Supplemental material
Supplementary materials can be found via https://doi.org/10.14730/aaps.2022.00752