Infrabrow excision with septo-myocutaneous flap repositioning in aged eyelids in Asians
Article information

Abstract
Asian eyelids are characteristically puffy, with a fold, and have bulging of the orbital fat and septum. Moreover, with the aging process, the orbital septum and skin lose elasticity and orbital fat atrophy proceeds, thus resulting in dermatochalasis and a sunken eyelid. We introduce a modified technique of infrabrow excision with septo-myocutaneous flap repositioning. An upper incision was made along the lower margin of the eyebrow and the placement of the lower incision was decided according to the amount of skin excision needed. After skin removal, the orbicularis oculi muscle (OOM) was incised 2 mm above the lower margin and dissected to expose the orbital septum. Additional dissection was performed along the preseptal plane to the supraorbital rim periosteum. Then, the lower flap (septo-myocutaneous flap) was anchored to the supraorbital rim periosteum. The overlapping OOM and subcutaneous layers were sutured separately. This technique makes it possible to correct the cause of an aging eyelid appearance. Additionally, an overlapping OOM aids in correcting sunken eyelids, and by tensioning the orbital septum, a puffy eyelid is corrected. As an advantage over the conventional infrabrow excision, our method prevents recurrence and corrects orbital septum laxity. Therefore, it can achieve more natural outcomes and lower recurrence rates.
INTRODUCTION
Asians have characteristically puffy eyelids due to bulging of the orbital fat and orbital septum. With aging, the main clinical manifestations are lateral hooding of the upper eyelid skin, sunken eyelids, and periorbital wrinkles due to orbital fat atrophy and laxity of the septo-myocutaneous layer [1]. Orbital fat protrudes due to septo-myocutaneous layer laxity, which worsens lateral hooding and sunken eyelids [2]. Infrabrow excision is a widely used surgical technique for correcting these aging processes. It has several advantages, especially rapid postoperative recovery and preservation of local anatomical features [3].
However, in certain patients, the degree of recurrence after infrabrow excision is unpredictable. Therefore, many surgeons have reported various techniques for overcoming this drawback, mostly regarding the preoperative design and manipulation of the orbicularis oculi muscle (OOM). Given the nature of the aging process, manipulation of the orbital septum is desirable. We presented the efficacy of our modified infrabrow excision procedure by repositioning a septo-myocutaneous flap. From May 2018 to February 2021, this modified procedure was performed in nine of 25 patients aged 32 to 82 years who underwent infrabrow excision. The chief complaint of all patients was loose eyelid skin. The study was reviewed and approved by the Institutional Review Board of Dankook University Hospital (approval no.: 2022-06-011). Written informed consent was provided by all patients; then, they were enrolled.
IDEA
Surgical technique
In the sitting position, an upper excision line was placed along the lower margin of the eyebrow. With the frontalis muscle relaxed and eyes closed, the upper eyelid and eyebrow were pulled upward, and the amount of skin to be removed was marked to design the lower excision line. The excisional range was designed within the medial margin of the eyebrow and less than 1 cm lateral from the lateral border.
Under local anesthesia using 2% lidocaine with 1:100,000 epinephrine, the incision was made with a no. 15 blade, 5 to 7 minutes after the hemostatic effect manifested. The upper incision was beveled to avoid injury to eyebrow hair follicles (Fig. 1A). After skin removal, the OOM was cut 2 mm above the inferior edge and dissected until the orbital septum was exposed (Fig. 1B). Then, the preseptal layer was dissected to expand the mobility of the lower flaps. The upper flap was also dissected along the preseptal layer to the supraorbital rim periosteum to fix the lower flap. To avoid nerve injury, the medial side was only minimally dissected at the time. Subsequently, the septo-myocutaneous layer of the lower flap, containing the orbital septum and the OOM, was lifted to the supraorbital periosteum and anchored with an absorbable suture material(polydioxanone 4-0; Johnson and Johnson MedTech) (Fig. 1C). The medial and lateral limbus and lateral canthus served as common anchoring points. We routinely used 3 points, but if necessary, 1 or 2 additional anchor points can be used (Fig. 1D). The edges of the incised muscle were minimally trimmed during these manipulations. Then, the patient was reseated to ensure that the proper changes were made. Finally, the overlapping OOM and subcutaneous layers were sutured separately with an absorbable suture material (Vicryl 5-0; Johnson and Johnson MedTech), and the skin was closed with a monofilament suture material (Prolene 6-0; Johnson and Johnson MedTech). If there was a concern regarding stepping due to the thin lower flap, a subcutaneous suture was performed vertically in the upper flap and horizontally in the lower flap. After 1 week, the skin suture material was removed.
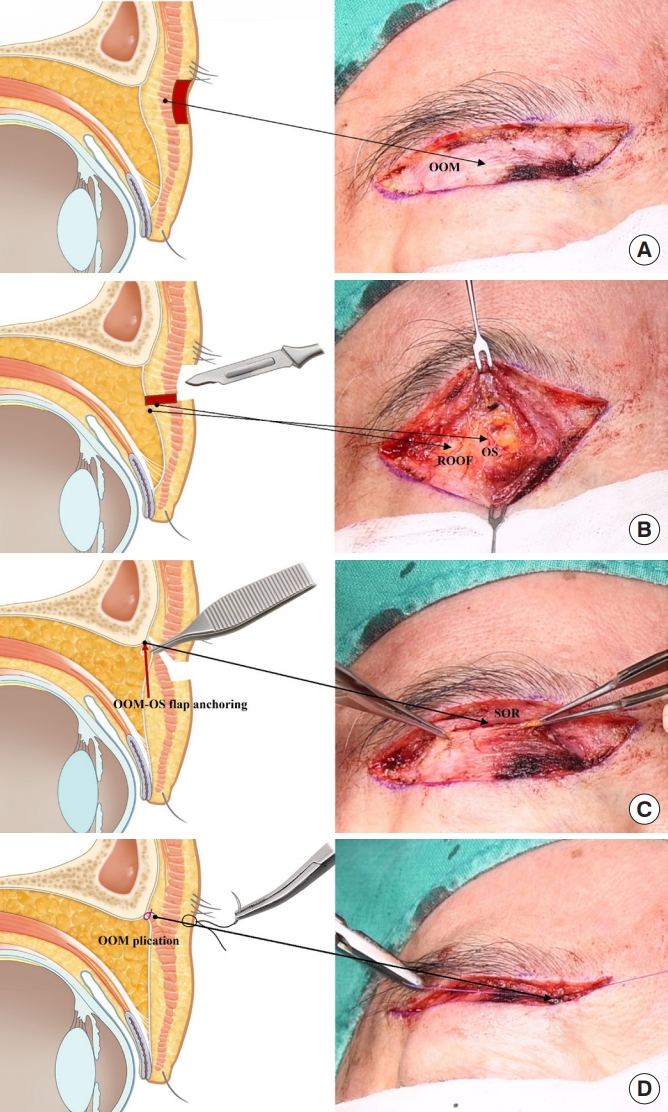
Schematic image and intraoperative photography of the surgical technique. The OOM was exposed after skin excision (A). An incision of the OOM was made 2 mm above the lower margin and dissected to expose the OS (B). The septo-myocutaneous flap (OOM and OS) was anchored to the supraorbital rim periosteum (C). The superior and inferior OOM flaps were overlapped (D). OOM, orbicularis oculi muscle; OS, orbital septum; SOR, supraorbital rim; ROOF, retro-orbicularis oculi fat pad.
Assessment
The surgical technique corrected the loose eyelid skin as well as the mild sunken status in patient 1. Additionally, decreased forehead wrinkles with preserved eyebrow position were observed at 3 months postoperatively (Fig. 2). Patient 2 showed improvement in her mildly puffy eyelid postoperatively and showed medium-term maintenance of her brow position (Fig. 3).
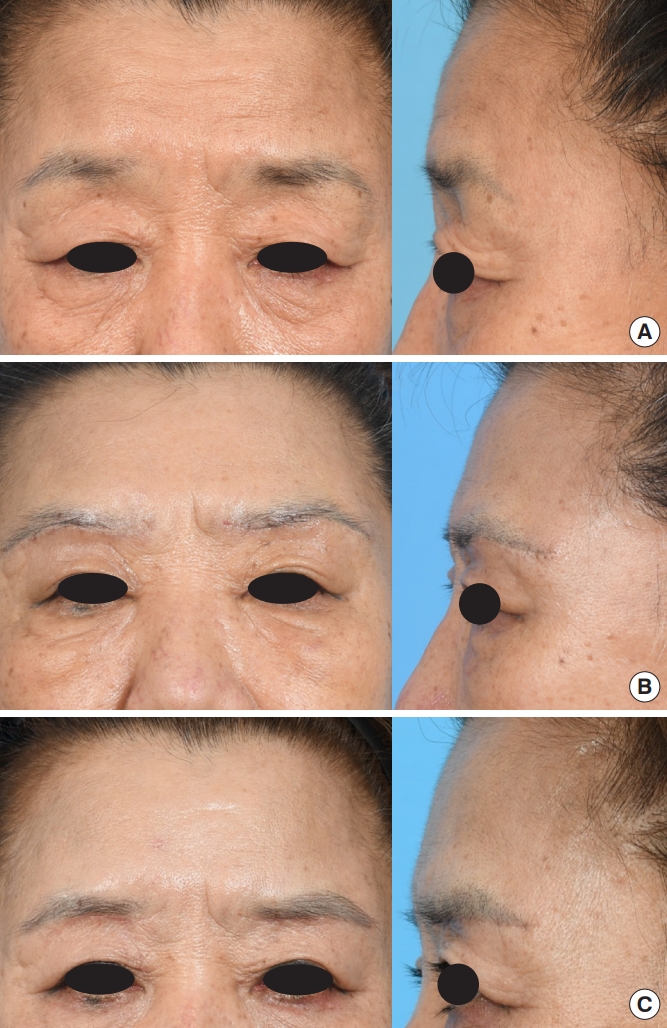
A 61-year-old female patient (patient 1) presented with loose eyelid skin and a mildly sunken status (A). These problems were fixed, and decreased forehead wrinkles with preserved eyebrow position were also observed and maintained at 10 days (B) and 3 months (C) postoperatively.
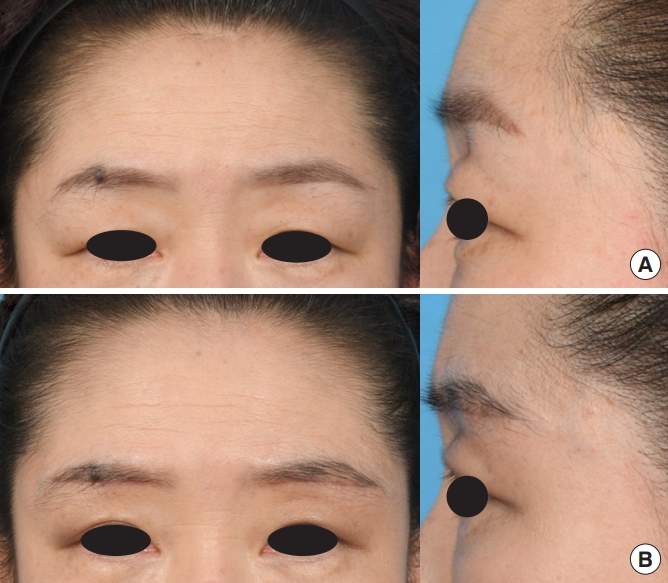
A 50-year-old female patient (patient 2) presented with loose eyelid skin and mildly puffy eyelid (A). At 2 months postoperatively, her mildly puffy eyelids had improved (B).
DISCUSSION
Differences between Asian and Caucasian eyelids stem from the lower dermal attachment of the levator aponeurosis. This causes both the orbital fat and orbital septum to descend, making the eyelid puffier. Aging is accompanied by fat atrophy and the loss of collagen and elastin with tissue laxity [4]. This process results in sunken eyelids, periorbital wrinkles, and laxity of the septo-myocutaneous layer, leading to orbital fat prolapse and lateral hooding in Asians [5]. The presence of attractive eyes is an important factor in recognizing the overall beauty of the entire face [6]. Regardless of race, wide-set eyes are considered beautiful, and those without fat pad protrusion or superior sulcus hollowing (that occurs with aging) are considered attractive [5]. Among many surgical techniques that make eyes more attractive, infrabrow excision is a widely used technique. Its advantages include rapid postoperative recovery, minimal swelling, and preservation of local anatomical features [1].
In an infrabrow excision, the upper incision is made along the lower margin of the eyebrow, and the lower margin is determined according to the amount of skin excision needed. There have been many modifications, but most were concerned with the preoperative design and OOM excision or manipulation (Table 1). Parkes et al. [3] first introduced the infrabrow excision procedure in 1976. They excised loose skin only. Moreover, in 2008, Kim et al. [7] performed an excision that was made deep enough to include the OOM in the lateral two-thirds. In 2014, Kim [8] presented the anchoring technique with the submuscular fascia to the supraorbital rim periosteum to alleviate crow’s feet deformity and reduce the risk of recurrence. Jin et al. [9] recently used the supraorbital OOM folding method for better eyebrow position. However, none of these methods mentioned orbital septum manipulation.
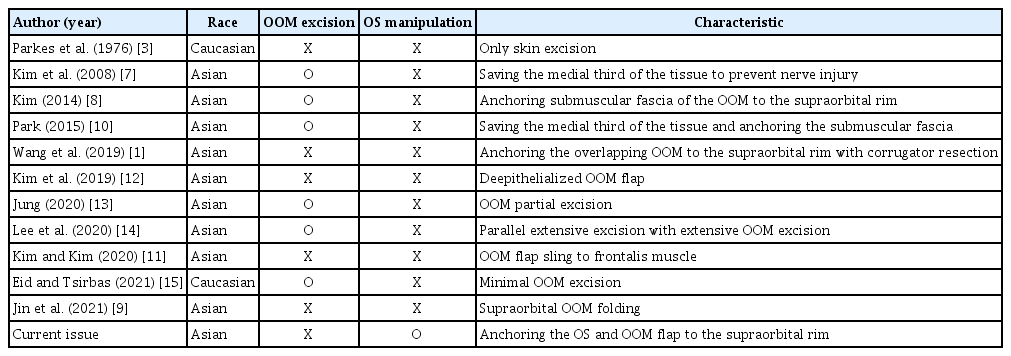
Analysis of papers that presented the performed surgical methods
With an understanding of the aging process, manipulation of the orbital septum is desirable. Sunken eyelids and orbital septum laxity can be corrected by anchoring the orbital septum to the supraorbital rim periosteum. Puffy eyelids, one of the main characteristics of Asian eyelids, can be corrected with this method by orbital septum tensioning. However, the degree of correction was limited practically; it was insufficient compared with fat grafting (for sunken eyelid correction) and fat removal (for puffy eyelid correction). Nonetheless, an advantage is that we minimized OOM injury, which is important since the OOM is the only muscle that closes the eye. This method also reduces the recurrence rate by anchoring the strong septum rather than loose skin or OOM. The overlapping OOM also helps correcting sunken eyelids. Meanwhile, this report had several limitations. Because of the small number of sampled patients, the effectiveness of this surgical technique was difficult to generalize. Furthermore, additional research on Caucasian populations is needed in the future.
In conclusion, we present a new technique of infrabrow excision with septo-myocutaneous flap repositioning. Rather than fixing the static submuscular fascia of the OOM to supraorbital rim periosteum, this method can achieve a more natural outcome and lower recurrence rate. Therefore, septo-myocutaneous flap repositioning can help to correct aged eyelids in Asians.
Notes
No potential conflict of interest relevant to this article was reported.
Ethical approval
The study was approved by the Institutional Review Board of Dankook University Hospital (IRB No. 2022-06-011).
Patient consent
All patients provided written informed consent for the publication and the use of their images.