INTRODUCTION
Breast augmentation mastopexy is a common procedure in cosmetic plastic surgery [1]. Augmentation mastopexy has proven to be a relatively safe operation, but Spear [2] stated that ŌĆ£disastrousŌĆØ complications such as skin flap necrosis and nipple loss can occur because of devascularization of the central breast. Although the probability of developing these serious complications is very low, if they do occur, methods to cover soft tissue defects should be considered. Reconstructing medium-sized, round soft-tissue defects on the breast with nipple loss is challenging due to aesthetic and psychological considerations for patients. Defects on the breast tend to be round due to the breastŌĆÖs shape, making reconstruction more difficult. The purse-string suture technique is simple to perform and produces satisfactory aesthetic outcomes in medium-sized soft tissue defects on the breast [3,4]. In addition, when combined with the Elsahy method, this technique can be used to repair and reconstruct inverted nipples [5,6]. If the nipple is completely lost, a local flap such as CV flap can be an excellent option. If the nipple has been successfully reconstructed, it is then possible to successfully reconstruct the nipple-areolar complex followed by areolar reconstruction through a skin graft or tattooing [7,8]. Herein, we report our experience of treating a patient with breast defects and nipple-areolar complex necrosis, in which aesthetically satisfactory outcomes were achieved through sequential reconstruction.
CASE REPORT
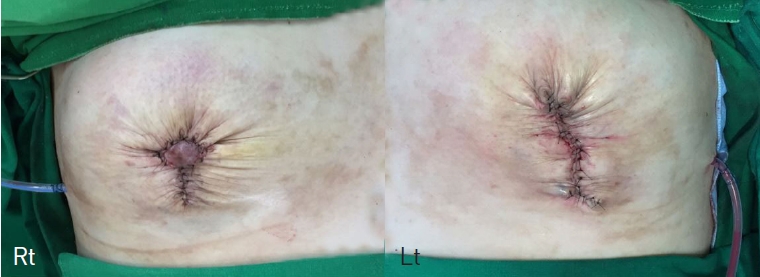
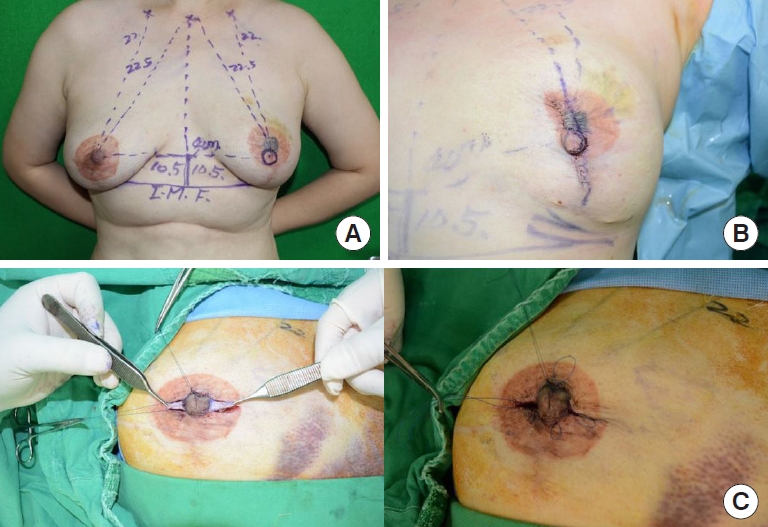
A 33-year-old woman underwent augmentation mastopexy and implant insertion through the periareolar approach on both breasts at a private clinic due to large and ptotic breasts. About 3 weeks after the procedure, she was referred to our outpatient department with soft tissue and nipple-areolar complex necrosis on the central parts of both breasts. Soft tissue necrosis with nipple partial loss had occurred on the right breast, as well as soft tissue necrosis with nipple total necrosis on the left breast, leaving a soft tissue defect measuring 4 ├Ś 4 cm on each breast. Therefore, both breasts required mound reconstruction. The nipple on the right side was partially preserved, but the nipple on the left side was completely lost, requiring surgery to create a new nipple (Fig. 1). Reconstructive surgery needed to be performed as soon as possible, because delayed reconstruction would lead to inferior aesthetic outcomes due to fibrosis and scar formation. The purse-string suture technique using polydioxanone (PDS) sutures #1-0 was applied to approximate the soft tissue defects and to maintain the shape of both breast mounds (Fig. 2). At postoperative 3 months, tattooing was simultaneously performed on both areolas (Fig. 3). The original reconstruction plan was to proceed with nipple reconstruction one side at a time at this time. However, due to the patientŌĆÖs social and psychological stress regarding surgery and fear of complications, only temporary tattooing was performed. Nonetheless, 8 months later, as the patient was preparing for marriage, she felt the need for nipple reconstruction and revisited the hospital for this purpose. Nipple reconstruction was performed through a vertically designed modified CV flap on the left breast at postoperative 11 months. At postoperative 12 months, inverted nipple repair using the Elsahy method and the purse-string suture technique on the right breast was performed (Fig. 4). Areolar reconstruction with tattooing was also performed sequentially. The breast mounds and nipple-areolar complexes on both sides showed symmetrical and satisfactory results (Fig. 5).
DISCUSSION
Breast augmentation is one of the most popular cosmetic procedures. Although augmentation mastopexy is not performed as frequently as augmentation or reduction mammoplasty alone, it is still a common procedure [1]. Augmentation mastopexy can be done in one or two stages, with two-stage surgery being considered safer. However, single-stage surgery is more convenient because it avoids the need for a second surgery [9]. Over time, single-stage augmentation mastopexy has been recognized as safe. For example, periareolar augmentation mastopexy was once the most litigated procedure in the United States, but related legal disputes have decreased in recent years [10].
According to Spear [2], when augmentation and mastopexy are performed together, blood flow to the central breast may be compromised due to a reduction in the skin envelope and an increase in soft tissue tension. The most serious complications that can result from diminished blood flow are soft tissue necrosis and nipple loss. However, Stevens et al. [9] reviewed 1,192 cases of augmentation mastopexy and found that these serious complications did not occur. While augmentation mastopexy is generally considered a safe procedure, it is important to be aware of and prepared for potentially disastrous complications. The original purpose of mastopexy was to correct sagging breasts. Mastopexy focuses on reshaping the breast, while augmentation focuses on increasing breast size. However, these procedures do not have to be performed separately and can be done simultaneously according to the patientŌĆÖs request and depending on the breast anatomy [10]. Therefore, an appropriate preoperative patient evaluation is crucial. Factors such as the patientŌĆÖs weight, height, and breast symmetry including size and shape, as well as the amount and quality of soft tissue, nipple and gland position, and symmetry of the nipple-areolar complex should be evaluated. The patientŌĆÖs expected postoperative results must also be fully understood [9,10].
As mentioned before, Stevens et al. [9] reported that augmentation mastopexy is a relatively safe procedure with a very low incidence of serious complications such as soft tissue necrosis and nipple loss. The risk of complications is higher if periareolar mastopexy is performed, the patient is a smoker, and saline implants are used. The most common complications are usually minor and manageable, such as poor scarring, delayed wound healing, implant deflation, and capsular contraction. However, it is important to note that serious complications such as soft tissue necrosis or nipple loss can occur at any time, and surgeons should be prepared to deal with such complications.
For defects that are relatively small, round, and located at the center of the breast, coverage using the purse-string suture technique can be considered [3,4]. The purse-string suture technique is known to have been first used in the 1950s by Dr. Bradford Cannon to repair surgical skin defects that occurred after tumor removal [3,11]. The purse-string suture is a type of subcuticular suture located within the dermis, and the suture continues around the entire circumference of the wound. The biggest advantage of this method is that it is easy and fast, yet leaves a relatively small scar, resulting in excellent aesthetic outcomes [3,12,13]. The purse-string suture technique is a useful method in reconstructing the nipple-areolar complex because it can create nipple projection and maintain it for a long time [12]. When reconstructing the breast, symmetry is the most important factor, and the same principle applies when reconstructing the nipple-areolar complex. Timing is critical in nipple-areolar complex reconstruction, which is usually planned 3 to 4 months after tissue stabilization following breast reconstruction. Historically, methods for nipple-areolar complex reconstruction included autologous tissue grafting and local flaps. Autologous tissue grafting produced successful projection results, but is currently not commonly used due to donor site morbidity. Various methods are now used, of which local flaps are the most common. Options include the Thomas flap (CV flap), skate flap, Bell flap, and so forth. Many methods have been developed by modifying these techniques for nipple-areolar complex reconstruction. The modified CV flap is a subdermal double local flap, which receives abundant blood flow from both sides and is advantageous for flap survival, resulting in better aesthetic outcomes [7,8].
A modified CV flap can be designed either vertically or horizontally. We chose the vertical design to preserve blood flow by making the scar-free area the base of the flap. Both the C and V flaps are raised in the deep dermal layer with preserved subcutaneous tissue, and the tip of the V flap is denuded and then folded into the reconstructed nipple [14]. Local flaps, including the CV flap, are an excellent method for nipple reconstruction, but a reduction in nipple projection due to natural contraction is inevitable [7,12,14]. To prevent nipple retraction and secure projection, the Elsahy method and the purse-string suture technique can be used during nipple reconstruction [6,12]. Elsahy method is a triangular areolar dermal flap used for correcting inverted nipples. In this method, triangular dermal flaps are designed on both sides of the nipple, followed by deepithelializing two skin flaps and then crossing these two dermal flaps through tunnels made at the bottom of the nipple. The opposite dermis is then sutured. Additionally, the nipple neck is tightened through the purse-string suture technique, which prevents nipple inversion during long-term follow-up [5,6]. We used these two methods together to reconstruct the remaining nipple-like remnant and successfully restore nipple projection.
It is important to remember that the nipple and areola form a complex and should be reconstructed together. The original color, shape, and position of the reconstructed areola should be restored to maintain symmetry. Skin grafting and tattooing are commonly used methods for areola reconstruction, and both methods are used in some cases [7,8]. Skin graft reconstruction has the advantage of mimicking the texture and fragmentation of the native areola, and the most common donor sites are the contralateral areola, inner thigh or groin, and labium. However, patients may not prefer this method because it is difficult to match the native areola perfectly and there is a risk of donor site morbidity. Tattooing is a relatively simple procedure compared to skin grafting and can match the original areola color completely through several retouches. Tattooing must be carried out in a sterile environment to prevent bacterial and viral transmission, and it is necessary to use skilled techniques that inject pigments neither too superficially nor too deeply. If only one side is tattooed, it should be tattooed darker than the contralateral areola, as the color will become lighter over time. It is also important to note that there may be a need for retouching, which can place a burden on the patient [7].
In conclusion, for medium-sized round defects in the center of the breast accompanied by nipple loss, the purse-string technique is a simple and effective reconstructive option that does not require additional incision or distortion of surrounding structures to maintain the shape of the breast mound. In addition to this technique, the modified CV flap and Elsahy method with tattooing can be used to successfully reconstruct the nipple-areolar complex and maintain its shape. Sequential reconstruction that considers shape, symmetry, color match, and scarring can lead to excellent aesthetic outcomes.