Changes in eyebrow position following blepharoptosis surgery
Article information

Abstract
Background
The position of the eyebrows is critical when planning blepharoptosis surgery. However, insufficient scholarly attention has been paid to the details of postoperative eyebrow height changes at each anatomical landmark. This study investigated the effect of blepharoptosis surgery on brow height and evaluated the change in brow position.
Methods
After a retrospective review of 247 patients, this study analyzed 53 patients (106 eyelids) who underwent levator and Müller’s complex advancement between March 2010 and January 2022. Brow heights were measured from the distance between the upper brow margin of each landmark and horizontal line of pupillary center on a digital photograph.
Results
The mean change of eyebrow lowering was 1.54 mm (P<0.001) at the medial canthus, 1.29 mm (P<0.001) at the medial limbus, 1.44 mm (P<0.001) at the center of the pupil, 1.40 mm (P<0.001) at the lateral limbus, 1.15 mm (P=0.001) at the lateral canthus, and 0.75 mm (P=0.021) at the lateral eyebrow end. The brow change was most prominent at medial canthus and least prominent at the lateral brow end. The preoperative brow position was only statistically significant factor predicting brow height descent after surgery according to multiple linear regression analysis (R2=0.305, B=–0.375, P<0.001).
Conclusions
The eyebrows lowered in most patients after blepharoptosis surgery. The preoperative brow position is the most important factor in predicting the change in brow height after blepharoptosis surgery.
INTRODUCTION
Eyebrows play a crucial role in expressing a person’s emotional state and conveying nonverbal information. They interact with multiple periorbital muscles, despite not being directly attached to the underlying bone [1]. While most body structures composed of soft tissues descend with age, the medial and mid-brow portions tend to elevate, resulting in an unnatural appearance. Generally, this paradoxical elevation of the eyebrow is observed in women as they age [2].
Blepharoptosis surgery, often performed for functional or cosmetic reasons, is one of the most common operations. This procedure corrects excessive skin and fat, typically when the upper eyelids are droopy or ptotic [3]. It is frequently noted in medical literature that patients with ptosis may elevate their eyebrows as a form of “compensation” for ptosis. Aging blepharoplasty or blepharoptosis surgery can reduce this compensatory action of the frontalis muscle, potentially leading to a lowering of the eyebrows. However, it is worth noting that eyebrow elevation can persist after ptosis correction. The specific characteristics of the relationship between eyebrow elevation and ptosis remain unclear [3].
Only a handful of studies have evaluated the impact of blepharoptosis surgery on brow height. However, there is currently no consensus regarding the surgery’s influence on brow position. This study aimed to determine the effect of blepharoptosis surgery on brow height and to evaluate changes in brow position.
METHODS
Patient selection
Informed consent for ptosis surgery was obtained from all patients, and this study adhered to the ethical principles outlined in the Declaration of Helsinki. We retrospectively reviewed 247 patients who underwent levator and Müller’s complex advancement between March 2010 and January 2022. Patient charts were reviewed for age, sex, marginal reflex distance (MRD1), levator and Müller’s complex advancement, and the presence of adequate preoperative and postoperative photographs. Patients with severe congenital ptosis that could not be corrected by levator and Müller’s complex advancement, those with facial nerve palsy, those who had received botulinum toxin injections, those lost to follow-up, and those with inadequate preoperative or postoperative photographs were excluded from the study. After reviewing the 247 patients, a total of 53 patients (106 eyelids) were ultimately included in this study. All operations were performed by a single senior surgeon who employed the same techniques for all patients.
Operation method
Skin incision lines were drawn 5 to 8 mm above the eyelash lines, and 2% lidocaine epinephrine (1:100,000) was administered along these lines. Using a #15 scalpel, skin incisions were made along the marked lines, and any excess skin and orbicularis oculi muscle were removed. Following this, the orbital septum was cut using monopolar electrocautery. Preaponeurotic fat pads were then separated from the underlying levator aponeurosis, and any surplus fat pads were excised. A small dose of lidocaine epinephrine was injected into the pretarsal levator aponeurosis, which was subsequently divided with electrocautery. Careful dissections were carried out between Müller’s muscle and the conjunctiva using bipolar cautery. Müller’s muscle and the levator complex were fully detached from the underlying conjunctiva. The Müller’s and levator complex were then moved caudally and secured to the tarsal plate with a Prolene 6-0 suture. The advancement length was approximately 2 to 3 times the amount of ptosis. The same procedures were performed on the upper eyelid of the opposite side. The remaining end of the advanced levator aponeurosis was trimmed, and the lower skin flap was attached to it. The upper skin flaps were then rearranged and the eyelid skin was stitched with a nylon 7-0 suture. The first central suture included the upper flap orbicularis oculi muscle to prevent triple folds, and the following sutures included only the cutaneous tissues. Skin tapes were placed on the upper eyelid skin 2 to 3 mm above the incision line to apply mild compression and facilitate natural fold formation.
Measurement method
Preoperative and postoperative photographs were taken of all patients. To ensure consistency in measurements, a 9-mm round marker was placed on the glabella of each patient as a reference point. Image J software (National Institutes of Health) was utilized for image analysis and the measurement of brow heights. There is no universally accepted standard for the optimal point of eyebrow position for measurement, although some studies have evaluated changes in eyebrow position by assessing the upper brow margin [2,4]. In our study, we used the upper brows to analyze changes in brow height following ptosis correction surgery. The upper eyebrow margins, which we defined as the highest starting point of hair, were determined based on the average positions indicated by two plastic surgeons. For patients with eyebrow tattoos, the upper eyebrow margins were defined as the highest starting point of the tattoo, rather than the eyebrow hair. The margin reflex distance (MRD1) was measured as the distance between the center of the cornea and the upper eyelid margin. Brow heights were measured as the distance between the upper brow margin at each brow point and the horizontal line, which is a line connecting both pupillary centers. Consequently, eyebrow heights at the medial canthus, medial limbus, pupillary center, lateral limbus, lateral canthus, and eyebrow lateral margin were measured (Fig. 1). MRD1 and each eyebrow height were measured both preoperatively and at least 6 months postoperatively (Fig. 2).

Sample of the method of measuring eyebrow height at eyebrow landmarks, using a reference green circle with a diameter of 9 mm for measurement. The red line represents the HL connecting the centers of both pupils. Yellow dots on each vertical blue line indicate the upper brow positions on each eyebrow landmark. MC, medial canthus; ML, medial limbus; PC, pupil center; LL, lateral limbus; LC, lateral canthus; LBE, lateral brow end; HL, horizontal line connecting the bilateral pupil centers.
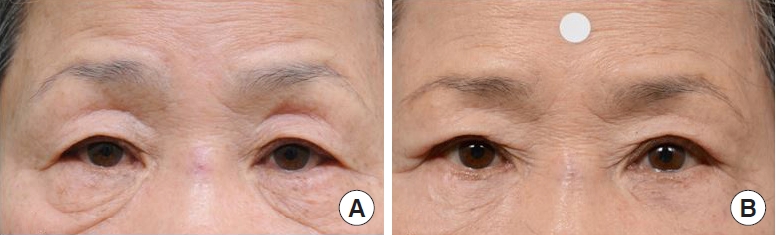
The eyebrow position was lowered after levator and Müller’s complex advancement surgery. (A) Before surgery and (B) 6 months after surgery.
Statistical analysis
Basic demographic data were compared using the paired t-test (for continuous variables). Both preoperative and postoperative eyebrow parameters were compared using the paired t-test for continuous variables, and the chi-square exact test for categorical variables. Pearson correlations were employed to evaluate the associations of preoperative brow position and preoperative MRD1 with changes in brow position and MRD1 post-surgery. The relationship between the change in brow position post-surgery and the preoperative brow and ptosis parameters was examined using multiple linear regression analysis to formulate a prediction equation. All statistical analyses were conducted using IBM SPSS Statistics ver. 22.0 (IBM Corp.). A P-value less than 0.05 was deemed to indicate statistical significance.
RESULTS
Fifty-three patients (106 eyelids) who underwent levator complex advancement upper blepharoptosis surgery were eligible for the study. The overall mean age of these patients at the time of their blepharoptosis surgery was 53.94 ± 18.98 years. The severity of ptosis was assessed using MRD1. The average preoperative MRD1 was 1.99 ± 1.64 mm, while the average postoperative MRD1 was 3.25 ± 1.17 mm. There was a significant increase in MRD1 following the correction of blepharoptosis (P < 0.001) (Table 1).

Summary of patient demographic characteristics
Out of the 106 eyelids that underwent blepharoptosis surgery, the eyebrow positions were observed to have lowered at various points. Specifically, this lowering occurred at the medial canthus in 76 eyelids (72%), at the medial limbus in 74 eyelids (70%), at the center of the pupil in 71 eyelids (67%), at the lateral limbus in 73 eyelids (69%), at the lateral canthus in 73 eyelids (69%), and at the lateral end in 68 eyelids (64%). There was no statistically significant difference in the rate of depression between these brow landmarks (P = 0.897) (Table 2).
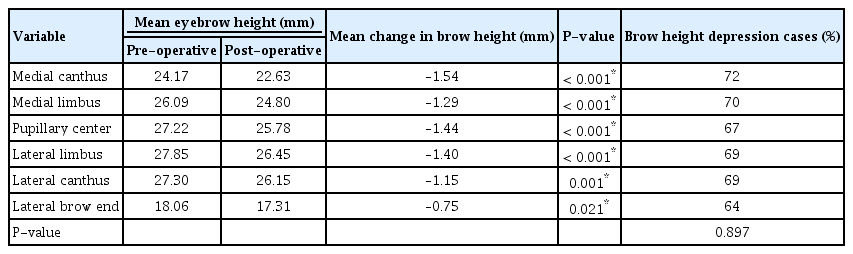
Eyebrow heights and changes at the preoperative examination and after blepharoptosis surgery at each eyebrow landmark (106 eyelids)
The mean lengths of eyebrow drooping across the 106 eyelids studied were as follows: 1.54 mm (P < 0.001) at the medial canthus, 1.29 mm (P < 0.001) at the medial limbus, 1.44 mm (P < 0.001) at the pupil’s center, 1.40 mm (P < 0.001) at the lateral limbus, 1.15 mm (P = 0.001) at the lateral canthus, and 0.75 mm (P = 0.021) at the lateral brow end. The greatest change in eyebrow position was observed at the medial canthus, while the smallest change was noted at the lateral brow end (Table 2 and Figs. 2, 3).

Preoperative and postoperative vertical eyebrow heights were measured from the horizontal mid-pupillary line. The numbers below the graph denote the mean difference in eyebrow height after blepharoptosis surgery at each eyebrow landmark. MC, medial canthus; ML, medial limbus; PC, pupil center; LL, lateral limbus; LC, lateral canthus; LBM, lateral eyebrow margin. *P<0.05, statistically significant.
The change in brow height following blepharoptosis surgery was found to correlate with the preoperative brow position (r = –0.55, P < 0.001). However, there was no correlation between the change in brow height and the preoperative MRD1 or the change in MRD1 post-surgery. A multiple linear regression analysis, which considered the change in brow height as a function of the preoperative brow position and preoperative MRD1, resulted in the following equation: Brow height change = 8.345–0.096 × preoperative MRD1–0.375 × preoperative brow position. This equation had an R2 value of 0.305 (P < 0.001). The only factor found to influence the eyebrow position after surgery, and thus predict the change in brow height following blepharoptosis surgery, was the preoperative brow position (P < 0.001) (Table 3 and Figs. 4, 5).
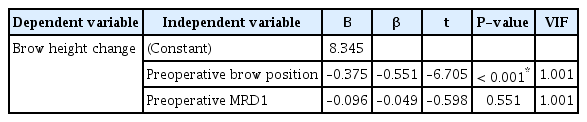
Predictive factors for eyebrow height descent after surgery based on multiple linear regression model analysis
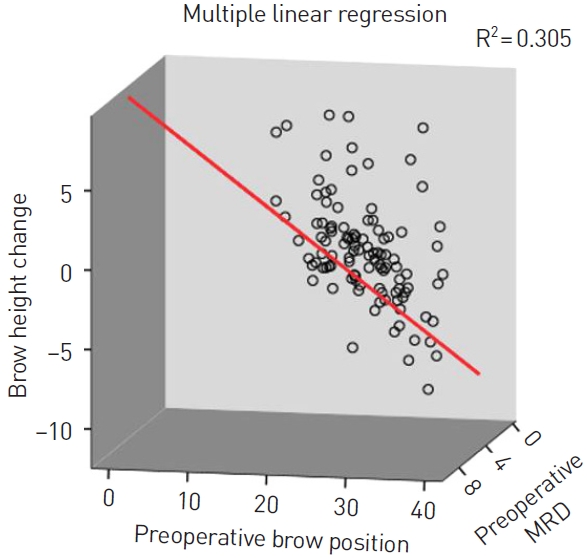
Brow height change related to preoperative brow position (independent variable) and preoperative MRD1 (independent variable) using the multiple linear regression model. The red line represents the linear line of best fit. Brow height change and preoperative brow position represent the average value at various landmarks of brow position. MRD1, marginal reflex distance.
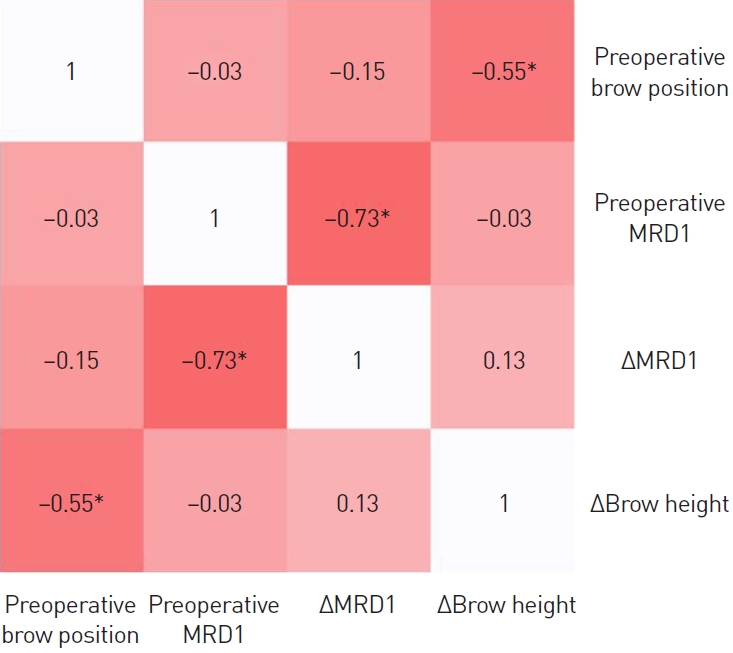
Correlation matrix between preoperative brow position, preoperative MRD1, change in MRD1 after surgery, and change in brow height after surgery. The color value of the cells is proportional to the strength of the associations, ranging from white (positive correlations) to red (negative correlations). Pearson correlation coefficients are shown in every cell. MRD1, marginal reflex distance. *P<0.05, statistically significant.
DISCUSSION
The eyebrow position results from an intricate balance between the muscles that depress and elevate it. The frontalis muscle serves as the sole elevator, while a group of muscles, including the corrugator supercilii, procerus muscles, depressor supercilii, and orbicularis oculi, function as depressors. It’s crucial to view the muscles in the brow area as a unified entity, given their interconnectedness and collective impact on the skin that overlays them. The four muscles—frontalis, prefrontalis, orbicularis oculi, and corrugator supercilii—do not independently facilitate skin movements. Instead, they always operate in concert, with each muscle influencing the others [1].
The relationship between eyebrow elevation and eyelid ptosis requires further understanding [5]. The position of the eyebrows tends to rise with age, particularly in the medial and middle segments [2]. As individuals age, the activity of the depressor brow muscle proportionally increases. Consequently, the frontalis muscle exhibits relative counterbalancing activity to the depressor muscle, leading to changes in brow height and shape [6].
The position of the eyebrow is a crucial consideration when planning upper blepharoptosis surgery. However, there remains ongoing debate about whether blepharoptosis surgery alters the position of the eyebrow, specifically in terms of elevation or depression. Only a handful of studies have examined the impact of blepharoptosis surgery on eyebrow position [7-12].
Dar et al. [10] assessed the impact of upper blepharoplasty on eyebrow height in 19 aging Caucasians by utilizing digital photographs. Their findings revealed no significant alteration in eyebrow height pre- and post-blepharoplasty. Similarly, Nakra et al. [11] evaluated the effect of upper blepharoplasty on brow position in a total of 19 patients, using clinical photographs. The change in brow position did not show any statistical significance in the patient who underwent upper blepharoplasty for simple dermatochalasis.
Conversely, some studies have shown changes in brow position [8,9,12]. Lee et al. [8] observed that, following blepharoptosis, the average eyebrow drooping distance across 60 eyelids was 2.81 mm at the inner canthus, 2.05 mm at the center of the pupil, and 1.13 mm at the outer canthus. The most significant drop in eyebrow position occurred at the medial canthus. Kokubo et al. [9] reported that the average eyebrow position was lowered following blepharoptosis with levator resection. The mean eyebrow drooping distance across 84 eyelids was 2.74 mm at the medial canthus, 2.91 mm at the pupillary center, and 2.58 mm at the outer canthus. The most pronounced drop was at the center of the pupil. In our study of 106 eyelids, the most significant descent in brow position was also at the medial canthus. When compared with our findings and those of Lee et al., the results are similar, with the greatest fall in eyebrow position occurring at the medial canthus. However, in the study of Kokubo et al., the most significant drop in eyebrow position was at the pupillary center.
There could be several reasons for the lowering of the eyebrow following blepharoptosis surgery. The frontalis muscle, the sole elevator of the eyebrow, plays a crucial role in determining eyebrow position. When the frontalis muscle contracts, the lower two-thirds of the muscle moves, primarily affecting the middle and inner portions of the eyebrows. The influence of the frontalis muscle extends laterally to the temporal fusion line of the skull. The lateral section of the frontalis muscle weakens over the fixation zone along the temporal margin. The lateral part of the forehead lacks an upward vector to counterbalance the downward gravitational force. This area has a lower resting tone of the frontalis muscle, providing less suspensory support for the lateral eyebrow [13,14]. Surgical correction of ptosis reduces the need to lift the brow by contracting the frontalis muscle [8]. Therefore, the post-surgical loss of frontalis muscle compensation could be the primary reason for the lowering of the eyebrow position, particularly in the medial canthus. In our study, we found that changes in the lateral end of the brow were relatively minor compared to other eyebrow landmarks, such as the medial canthus and medial limbus. The relatively weak anatomical support and force vector on the lateral brow, compared to the medial brow, could result in relatively minor changes in brow position following blepharoptosis surgery.
The decrease in weight of the external eyelid following surgery could potentially lead to a lowering of the eyebrow position. The position of the eyebrows is influenced by the weight of the eyelids. A weighted eyelid, including in instances of unilateral weighted eyelid, can cause both the ipsilateral and contralateral eyebrows to elevate due to the contraction of the frontalis muscle [15].
The corrugator supercilii is primarily distributed in the medial canthus, and its activity tends to increase with age [6]. The frontalis, in comparison to the corrugator supercilii, may be relatively weakened, which could persist even after blepharoptosis surgery. This could lead to an imbalance in eyebrow position, potentially contributing to the lowering of the medial eyebrow rather than the lateral eyebrow post-surgery.
In terms of upper blepharoplasty, surgical limitations may result in less height change in the lateral brow compared to the medial brow. As the aging process progresses, excessive skin on the lateral eyelids can lead to skin hooding. It has been challenging to correct lateral hooding using only classic upper blepharoplasty; even when corrected, this method often results in an unattractive scar beyond the lateral canthus [16-18]. To achieve the best aesthetic outcomes, including addressing lateral skin hooding, there are numerous types of skin incisions, ranging from elliptical to trapezoid, depending on the surgeon’s preference [19-22]. Some surgeons argue that the skin incision should not extend beyond the lateral orbital rim in order to conceal the scar within a natural skin fold [20]. Given these factors, it is possible that eyebrow drooping may be less noticeable in the lateral brow following blepharoptosis correction surgery, as observed in our study.
We assessed the impact of blepharoptosis surgery on eyebrow position by measuring MRD1 and brow heights both pre- and post-operation. Our study revealed a significant correlation between preoperative brow position and postoperative brow height change. However, no significant correlation was found between MRD1 and changes in brow height. To forecast surgical outcomes, we formulated the following equation: brow height change = 8.345–0.096 × preoperative MRD1–0.375 × preoperative brow position. The preoperative brow position was the sole influential factor (P < 0.001) in predicting brow height changes post-surgery, rather than the degree of ptosis. For patients undergoing levator and Müller’s complex advancement surgery, preoperative brow position measurement appears to be a useful predictor of brow depression outcomes following ptosis surgery.
There are some limitations in our study. We did not analyze the preoperative and postoperative levator function of the patients in our study due to the retrospective nature of the chart review. It would have been beneficial to analyze the levator function both before and after surgery, given that we performed levator and Müller’s complex advancement during the operation. Another limitation of our study is the lack of data on the amount of skin excision. Some studies suggest that the removal of eyelid skin can also contribute to the lowering of the eyebrow [9,23]. It has been suggested that eyebrow descent is better achieved with skin excision rather than levator resection alone [9]. Therefore, a future prospective study should include both levator function and skin excision to evaluate their relationship with changes in eyebrow height after levator and Müller’s complex advancement surgery. Additionally, our study had minor limitations such as a relatively small sample size, and we did not consider differences in brows between males and females, or analyze brow differences across different age groups.
In conclusion, the eyebrow position was lowered in most patients who had blepharoptosis surgery. The greatest changes in eyebrow position after blepharoptosis surgery were observed in the medial canthus (1.53 mm) and the least (0.75 mm) in the lateral brow end. The preoperative brow position is vital in predicting the brow height change after blepharoptosis surgery.
Notes
No potential conflict of interest relevant to this article was reported.
Ethical approval
This study was approved by the Institutional Review Board of Korea University Ansan Hospital (IRB No. 2023AS0094) and performed in accordance with the principles of the Declaration of Helsinki.
Patient consent
The patients provided written informed consent for the publication and the use of their images.