Combined, Minimally Invasive, Thread-based Facelift
Article information
Abstract
Background
As society changes, patients have high expectations of plastic surgery and rapid recovery after surgery. A thread-based facelift meets these requirements and is growing in popularity.
Methods
Former thread lifts were either floating or fixed types. The authors used both types. Using a vertical line from the lateral orbital rim as the center, the anterior face was lifted with floating-type threads and the lateral face was lifted with fixed-type threads. The Blue RoseTM thread was used for the combined-type facelift, as it is stronger than other threads. Improvements were measured using the Global Aesthetic Improvement Scale (GAIS).
Results
Eighteen patients out of 28 were followed over 3 months. Five patients (28%) reported a GAIS score of 2, 10 patients (55%) had a GAIS score of 3, 2 patients (11%) had a GAIS score of 4, and one patient was unsatisfied with the surgical results. Results showed improvements in 83% of the patients.
Conclusions
The combined, minimally invasive, thread-based facelift has some benefits. First, the functional anatomy of the face is considered. Second, the pulling force of the threads is stronger than formerly used threads. Third, especially in Asian patients, the postoperative broadening of the malar area can be minimized. Thus, a combined thread lift using Blue Rose threads can provide a natural-looking and strong facelift.
INTRODUCTION
Aging is a natural, biological process. Patients want to overcome the aesthetic problems associated with facial aging. Plastic surgeons have tried facelifts to meet patients’ expectations [1,2]. With the development of society and technology, patients prefer simple, less-invasive procedures for rapid recovery. A barbed suture lift can meet the requirement for a minimally invasive facial rejuvenation procedure.
Former thread lifts have used either a floating or fixed type thread [1]. But when we consider the functional anatomy of the face in terms of facial expressions and mastication, and a natural looking appearance after surgery, a floating-type thread lift is preferred for the mobile area of the face and a fixed-type thread lift is recommended for use in relatively fixed areas. The authors call this method the combined-type thread lift. The authors have performed this type of facelift in 28 patients with satisfactory results.
METHODS
Mendelson et al. [3,4] classified the region of the face into the mobile anterior face involved in facial expressions and the fixed lateral face overlying masticatory structures (Fig. 1). The retaining ligaments are located on a vertical line from the lateral orbital rim, which divides the anterior and lateral face.

A vertical line from the lateral orbital rim divides the face into the mobile anterior and fixed lateral regions.
We drew a vertical line from the lateral orbital rim (shown in Fig. 2) and applied a fixed-type thread at a point lateral to the line. Hair was shaved around the slit incision sites. The rounded needle with thread entered the incision site and was anchored in the deep temporal fascia. The central portion of a 43 cm-sized, Blue Rose™ thread was anchored in the deep temporal fascia, using the same method. The threads pull soft tissue toward four predetermined points (Fig. 2A and C).
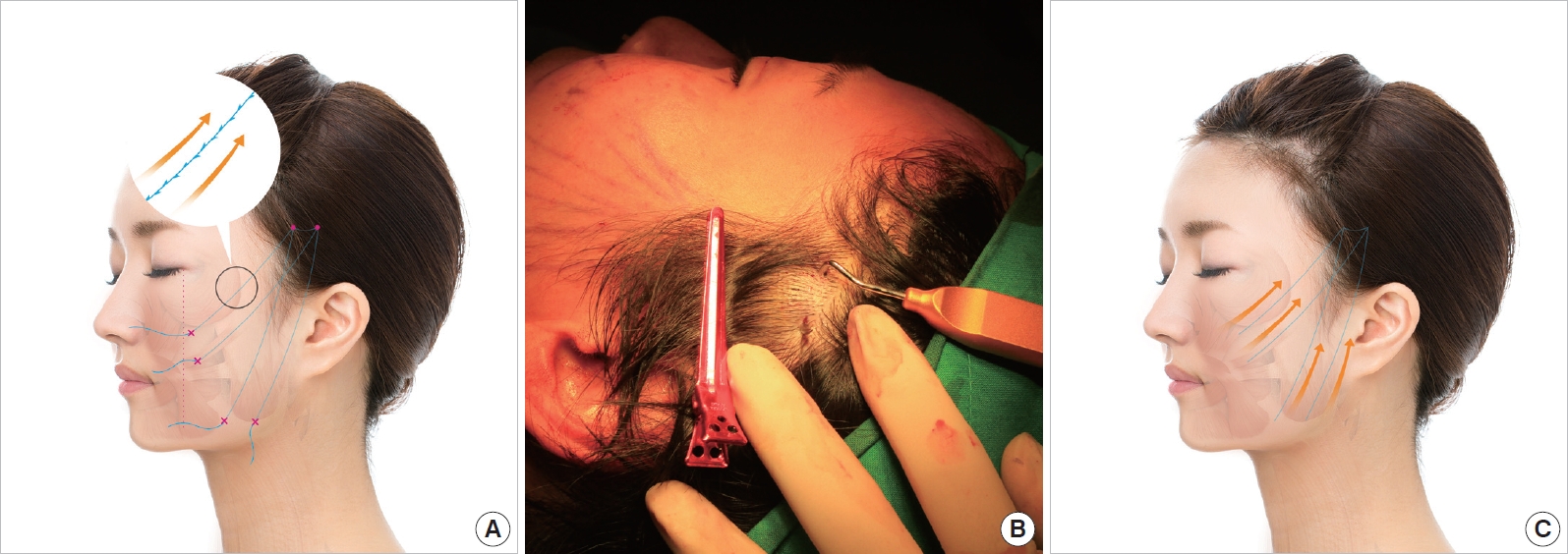
Fixed-type lift for the lateral face. (A) A red dotted line divides the face into the anterior and lateral regions. The thread was inserted (red dots) and pulled (red X) through the holes made by the needle, and both ends of the thread were fixed. Yellow arrows indicate the unidirectional, barbed sutures. (B) The ptotic soft tissues were lifted toward the deep temporal fascia by a rounded needle. (C) The vector of the force (yellow arrows) was toward the temporal area.
Next, the floating-type threads (17 cm-sized Blue Rose thread) are inserted to lift the ptotic anterior face from the hair line (Fig. 3A and B). These threads gather the soft tissues and pull the ptotic soft tissue from the bottom. Fig. 4 shows the immediate postoperative photo before cutting the ends of the threads.

Floating-type lift for the anterior face. (A) The bidirectional, barbed threads are shown (yellow arrows). (B) The soft tissues were gathered toward the midline. Yellow arrows show the vector of the force. The ptotic soft tissues on lower portion were lifted.

Before cutting the end of the fixed-type threads, the ends exited the inferior and medial sides. Floating-type threads are shown in the entrance. The ends of the threads were pulled appropriately and cut so as not to expose the threads.
Improvements reported by the patients were investigated using the Global Aesthetic Improvement Scale (GAIS; Table 1) [5]. The preoperative and postoperative photos were assessed using GAIS by a third-party physician who was not involved in the operation.
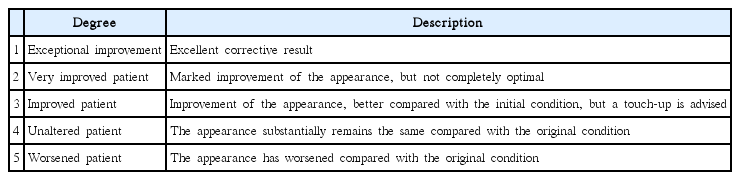
Global Aesthetic Improvement Scale (GAIS)
RESULTS
Patient demographics are summarized in Table 2. Eighteen patients out of 28 were followed for over 3 months. Assessments were made using postoperative photos and defined by GAIS score. Five patients (28%) had a GAIS score of 2, 10 patients (55%) had a GAIS score of 3, 2 patients (11%) had a GAIS score of 4, and one patient was unsatisfied with the surgical results. This patient received an additional facelift.

Patient demographics
No major complications were reported during the follow-up period. Some minor complications, including skin dimples by the strong pulling force during the thread cutting section, were observed. Minor complications that developed during the early postoperative period were improved by massage.
Case 1
A 26-year-old female visited our outpatient clinic complaining of soft tissue drooping after a facial contouring surgery. She received the combined facelift surgery and was satisfied with the results at the 3-month postoperative follow up (Fig. 5).

(A) Preoperative photograph of the 26-year-old patient who complained of soft tissue drooping. (B) Postoperative photograph at 3 months in which the degree of soft tissue drooping was much improved.
Case 2
A 56-year-old female, who showed facial soft tissue sagging, was unable to get a standard facelift performed for personal reasons. She underwent a thread-based facelift instead. She was received follow-up examinations at 7 days and 3 months. At the 7-day follow up, there were some local dimples on her face due to an imbalance between the pulling forces. These dimples were improved at the 3-month follow up. The cosmetic result was a natural looking face (Fig. 6).

(A) Preoperative photographs of the 56-year-old female. (B) On postoperative day 7, there were some lines and dimples on the face. (C) By 3 months, the patient had a natural looking appearance. Although there was an abundance of soft tissue in the lower face, she was satisfied with the final results without the need for additional procedures.
DISCUSSION
Facelifts using barbed sutures were introduced by Sulamanidze in the late 1990’s [1]. Both thread-based and other surgical methods were subsequently developed. The early, multi-dented, bidirectional suture was of the floating type that gathered tissues in the middle of the suture without anchorage at either end [6]. Unidirectional sutures were then introduced to enhance stability by anchoring both ends at fixed points [7]. Recently, absorbable and nonabsorbable sutures of various lengths and shapes and sizes of needles have been used for other regions of the face [8].
Most previous reports have dealt with only the floating or fixed type of thread lifting [1,7]. The authors used combined thread lifting and achieved postoperative improvements in 83% of the patients.
The combined method has some benefits. First, the face is divided into the mobile anterior and fixed lateral regions. If lifted with a fixed-type thread, the anterior face would display an awkward expression. With floating-type thread lifting, however, natural animation is possible. Second, the pulling force of the floating-type thread is not enough strong to achieve satisfactory results. However, the ptotic soft tissue of the anterior face can be lifted and the strength maintained via connection to a fixed point in the lateral face. Third, the malar area was broadened after the use of fixed-type thread lifting in Asian patients. Using the author’s method, the tissues were retained in the central region of the suture using a floating-type thread and the malar area was not broadened (Fig. 7). Fourth, barbed thread is known to have cuts in the cylinder-shaped thread, which weakens the tension of the thread, because the diameter of the cut area is decreased. Blue Rose thread has dents but not cuts, which protrude from the cylinder-shape thread and is strongly anchored in the tissue.

The left side of the patient shows the broadened malar area due to the lateral lift by the fixed-type thread. On the right side of the patient, a floating-type thread retains the tissue in the central region of the thread and prevents malar area broadening.
The authors believe that combined type lifting is much more effective than former thread lifting. The absorbable suture used in the present study contains polydioxanone, and thus the lift cannot be sustained for a long time. It results in a natural looking appearance, but maintenance of the lift is compromised.
However, thread lifting with absorbable suture is expected to find wide application, as Botox and filler injections have become popular procedures despite their disadvantages. Absorbable sutures are safer than nonabsorbable sutures, considering that the removal of the nonabsorbable filler is difficult.
The final results of thread-based lifts can only be evaluated subjectively. Thus, the effects of variables such as skin type, race, age, and history of smoking on final outcomes can be discussed as complications. Rachel et al. [9] reported that the incidence of complications or early recurrence was independent of patient age, type of thread, or technique. In the present study, the effects of such variables to the results were not evaluated, due to the small size and the short-term follow up. Further studies should address these points.
The limitations of the present study are the short term follow-up period and the small number of cases. The assessment scale depends on subjective factors. Long term follow-up results with more objective assessment criteria are thus needed.
Acknowledgements
The Catholic Institute Review Board approved our study.
Notes
No potential conflict of interest relevant to this article was reported.